


11 April, 2023 by Shahriar Lahouti.

Approach to crashing patients on mechanical ventilation
There are multiple reasons for a patient to deteriorate while on mechanical ventilation. Having a systematic method of evaluating this deterioration is the best way to identify and fix the underlying problem. For patients who develop sudden respiratory distress or hemodynamic instability on mechanical ventilation, the following diagnostic and therapeutic algorithm can be used.
Clinical features of crashing patients (cardiac arrest/near arrest)
- New unexplained and rapidly dropping SBP < 80 mmHg, rapidly desaturating to SaO2<80%, extreme bradycardia or tachydysrhythmias, cardiac arrest while on mechanical ventilation.
Differential diagnosis
-
Keep in mind the “DOPES” mnemonic to rapidly consider the primary etiologies of the crashing ventilated patients 1:
-
D: Displaced tube, dysrhythmias
-
O: Obstructed tube
-
P: Pneumothorax
-
E: Equipment malfunction
- S: Stacked Breaths (Auto-PEEP).
-
Management
- Immediately disconnect from ventilator (this also allows for expiration of stacked breaths).
- Give manual bag ventilation with oxygen 100%.
- Bagging should be given by the provider but not anyone else, because this lets you get a sense of what the potential problem is (resistance to bagging).
- Pay particular attention to the delivery of manual ventilation. Limit the respiratory rate to 8 to 10 breaths/min.
- Excessive rates will increase intrathoracic pressure and lead to a decrease in venous return and cardiac output
- Look at ETT and ensure it is the same level it was at when it was put in.
- Listen for the air leaks from cuff rupture or cuff above the cords and feel for cuff leak.
- Feel the pressure of pilot balloon of endotracheal tube, and how is the patient bagging (Difficult to bag or too easy to bag).
-
If the patient improves when disconnected from the ventilator, it is likely an equipment (ventilator) or ventilator setting etiology.
-
If the patient has a long expiration after being disconnected from the ventilator and then stabilizes, consider auto positive end-expiratory pressure (PEEP) as the etiology (breath stacking).
-
- If respiratory distress or hemodynamic instability persists despite disconnecting the patient from the ventilator and ventilating with 100% oxygen via a bag valve mask:
-
Evaluate for the following life-threatening conditions and treat accordingly.
- Obtain a focused history, exams and imaging
- History: Indication for intubation? Difficulty of the intubation? Depth of the ET tube? Ventilator settings? Recent procedures or moves (central line insertion; chest tube placement; removal or transition to a water seal; thoracentesis; ET tube manipulation; transport off the stretcher; rotation for cleaning, a procedure, or chest radiography).
- Bedside ultrasound, CXR?
- Current oxygen saturation and end-tidal CO2?
- Life-threatening causes
- Tension pneumothorax: Consider needle decompression followed by tube thoracostomy placement
-
Large pleural effusion: Consider therapeutic thoracocentesis.
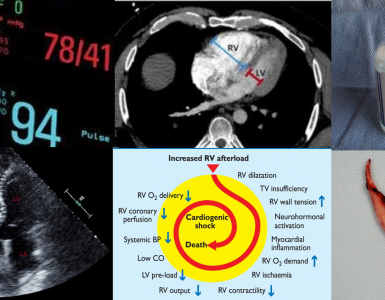
- Pulmonary edema (cardiogenic): Elevated head of the bed at 45 degrees, reduce afterload, +/- diuretics
- Obtain a focused history, exams and imaging
- In the absence of life-threatening condition, assess for resistance to bagging.
- If bagging is difficult: Consider ETT obstruction and try to pass suction catheter.
- If it is difficult to pass down: ETT obstruction (see the below algorithm for further management).
- If easily passes through: Consider a trial of sedation, paralysis and then reassess resistance to bagging (proceed as per following algorithm).
- If easy bagging, consider air leak. Evaluate by capnography and cuff pressure. May need ETT replacement.
- If bagging is difficult: Consider ETT obstruction and try to pass suction catheter.
-
Algorithm

👉For nearly stable or slowly deteriorating patients on ventilation, see here.
Going further
- Vent Management in the Crashing Patient with Haney Mallemat (REBEL EM)
- Endotracheal Tube Cuff Leaks and Tube Exchanges (EMCrit)
References
- Monica E. Kleinman et al. Pediatric Advanced Life Support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. AAP. 2010
- Roberts JR, Hedges JR. (2018). Roberts and Hedges’ Clinical Procedures in Emergency Medicine E-Book: Elsevier Health Sciences.


Add comment