
12 June 2026 via Shahriar Lahouti. Peer-reviewed by Mojtaba Chardoli.
CONTENTS
- Preface
- Essentials for GI US
- Inflammatory Bowel Disease Ultrasound
- RECAP
- Going further
- Guidelines
- Appendix
- Media
- References
Click to expand/collapse abbreviation list
| Abbreviation | Full Term |
|---|---|
| 5-ASA | 5-Aminosalicylic Acid |
| ACG | American College of Gastroenterology |
| ASCA | Anti-Saccharomyces cerevisiae Antibodies |
| ASUC | Acute Severe Ulcerative Colitis |
| AZA | Azathioprine |
| BUSS | Bowel Ultrasound Score |
| BUS | Bowel Ultrasound |
| BWT | Bowel Wall Thickness |
| CD | Crohn’s Disease |
| CDAI | Crohn’s Disease Activity Index |
| CDEIS | Crohn’s Disease Endoscopic Index of Severity |
| CDI | Color Doppler Imaging |
| CEUS | Contrast-Enhanced Ultrasound |
| CMV | Cytomegalovirus |
| CRP | C-Reactive Protein |
| CT | Computed Tomography |
| CTE | Computed Tomography Enterography |
| EAUS | Endoanal Ultrasound |
| ECCO | European Crohn’s and Colitis Organisation |
| EFSUMB | European Federation of Societies for Ultrasound in Medicine and Biology |
| ERUS | Endorectal Ultrasound |
| ESGAR | European Society of Gastrointestinal and Abdominal Radiology |
| FC | Fecal Calprotectin |
| GI | Gastrointestinal |
| GIUS | Gastrointestinal Ultrasound |
| HBI | Harvey-Bradshaw Index |
| IBD | Inflammatory Bowel Disease |
| IBUS | International Bowel Ultrasound Group |
| IL | Interleukin |
| IUS | Intestinal Ultrasound |
| JAK | Janus Kinase |
| MES | Mayo Endoscopic Score |
| MHz | Megahertz |
| 6-MP | 6-Mercaptopurine |
| MRE | Magnetic Resonance Enterography |
| MRI | Magnetic Resonance Imaging |
| MTX | Methotrexate |
| MUC | Milan Ultrasound Criteria |
| NUDT15 | Nudix Hydrolase 15 |
| pANCA | Perinuclear Anti-Neutrophil Cytoplasmic Antibody |
| POCUS | Point-of-Care Ultrasound |
| PRO | Patient-Reported Outcome |
| PRO2 | Patient-Reported Outcome 2 (stool frequency + abdominal pain) |
| PSC | Primary Sclerosing Cholangitis |
| RCT | Randomized Controlled Trial |
| SC | Subcutaneous |
| SES-CD | Simple Endoscopic Score for Crohn’s Disease |
| SICUS | Small Intestine Contrast Ultrasound |
| S1P | Sphingosine-1-Phosphate |
| STRIDE | Selecting Therapeutic Targets in Inflammatory Bowel Disease |
| SUS-CD | Simple Ultrasound Score for Crohn’s Disease |
| SWE | Shear Wave Elastography |
| TABS | Transabdominal Bowel Sonography |
| TAUS | Transabdominal Ultrasound |
| TH | Transmural Healing |
| TI | Terminal Ileum |
| TNF | Tumor Necrosis Factor |
| TPMT | Thiopurine Methyltransferase |
| TPUS | Transperineal Ultrasound |
| UC | Ulcerative Colitis |
| UCEIS | Ulcerative Colitis Endoscopic Index of Severity |
| US | Ultrasound |
| VCE | Video Capsule Endoscopy |
| VTE | Venous Thromboembolism |
Preface
Ultrasonography is frequently used to diagnose various gastrointestinal diseases, in both acute and chronic settings. Its non-invasiveness, lack of ionizing radiation, low cost, and real-time capabilities make it an ideal first-line imaging tool.
Clinical implications of bowel ultrasound include its use as part of a routine abdominal scan for a broad range of non-specific abdominal symptoms, and its dedicated role in assessing acute conditions such as appendicitis, diverticulitis, intestinal obstruction, and perforation, as well as chronic gut-related disorders (discussed separately). In patients with Crohn’s disease, ultrasound contributes to the detection of disease, evaluation of its extent, identification of complications such as abscesses, fistulas, obstructions, and assessment of disease activity and follow-up.
Beyond detecting inflammation, IUS helps differentiate active disease from functional symptoms—a common clinical dilemma, as up to 60% of IBD patients have chronic pain and ~33% of those in remission report IBS-type symptoms (more on this here).
This article discusses the utility of ultrasound in inflammatory bowel disease.
Essentials for GI Ultrasound
Anatomy
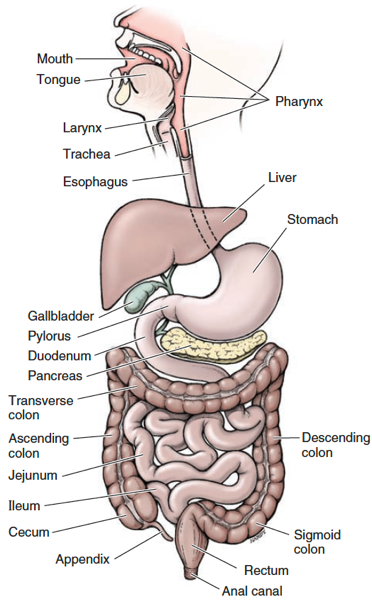
◾️Small bowel
- Between stomach and large intestine
- ~ 4-7 meters in length
- Centrally located in abdomen
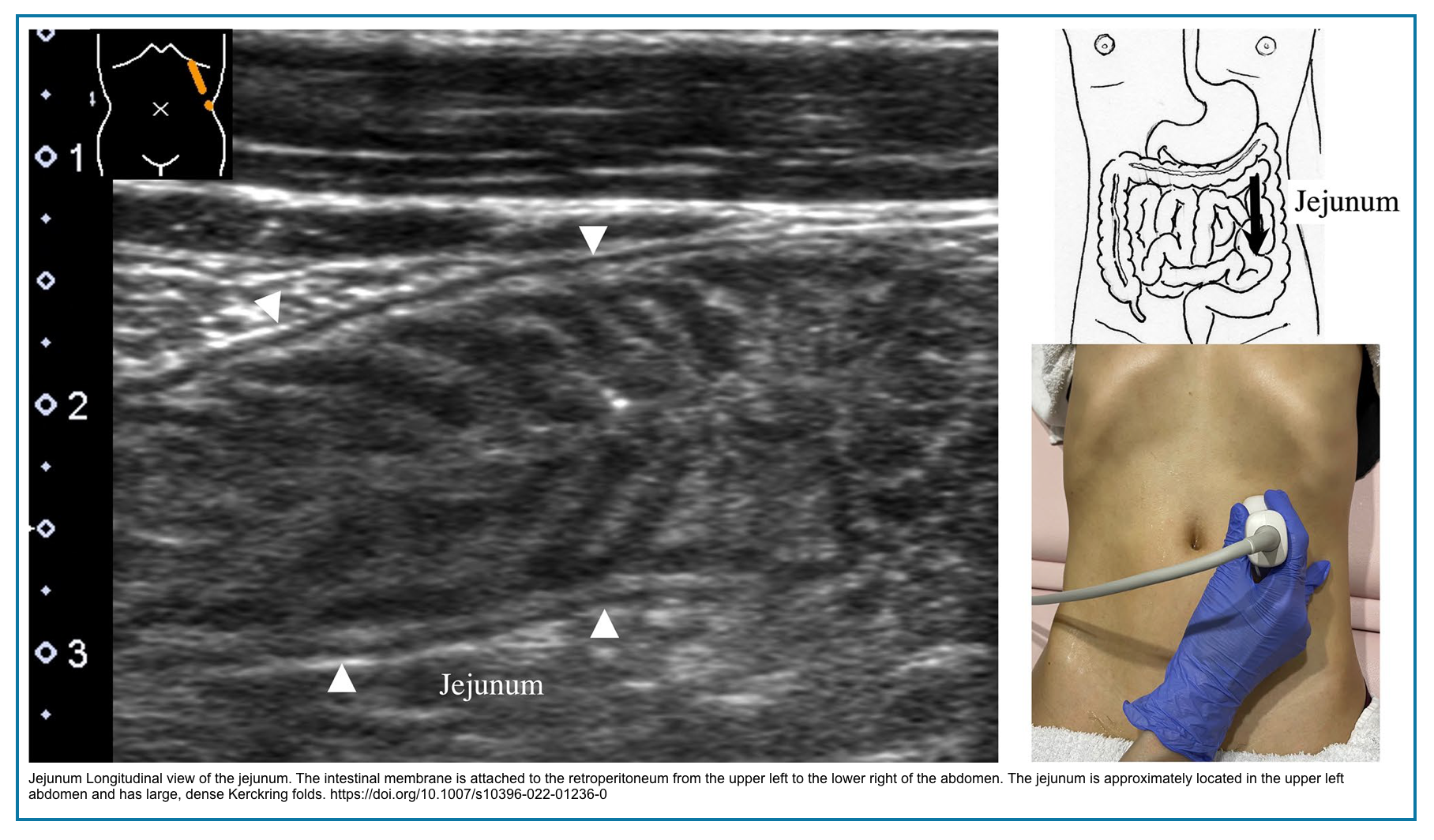
- Contents of jejunal loops are usually liquid and appear hypoechoic/anechoic.
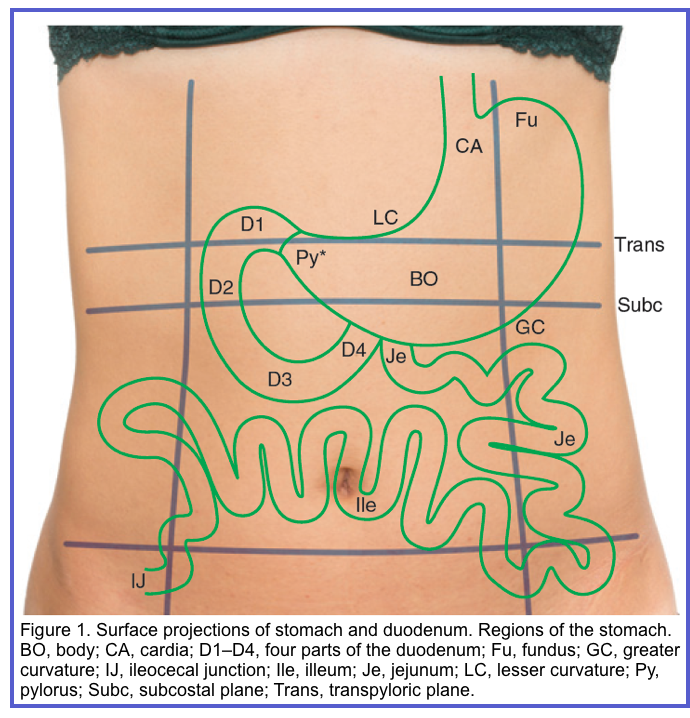
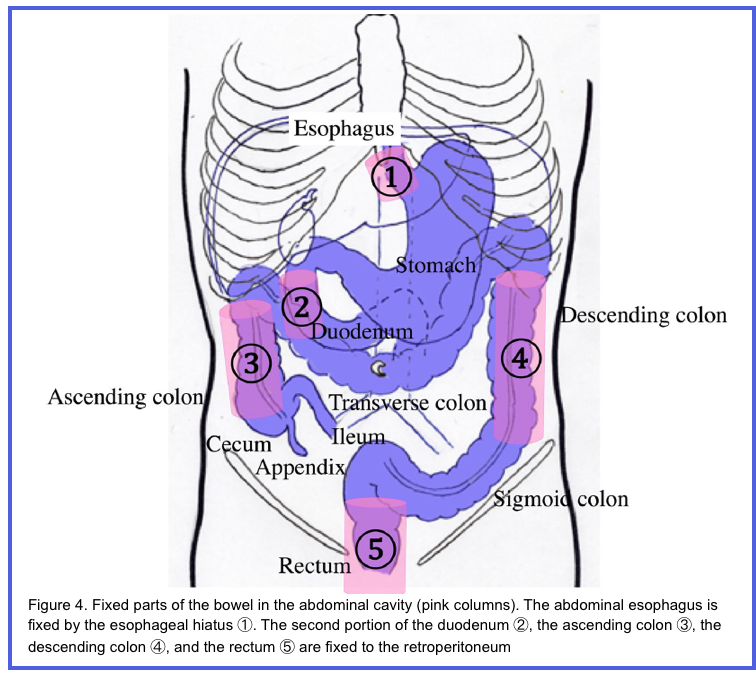
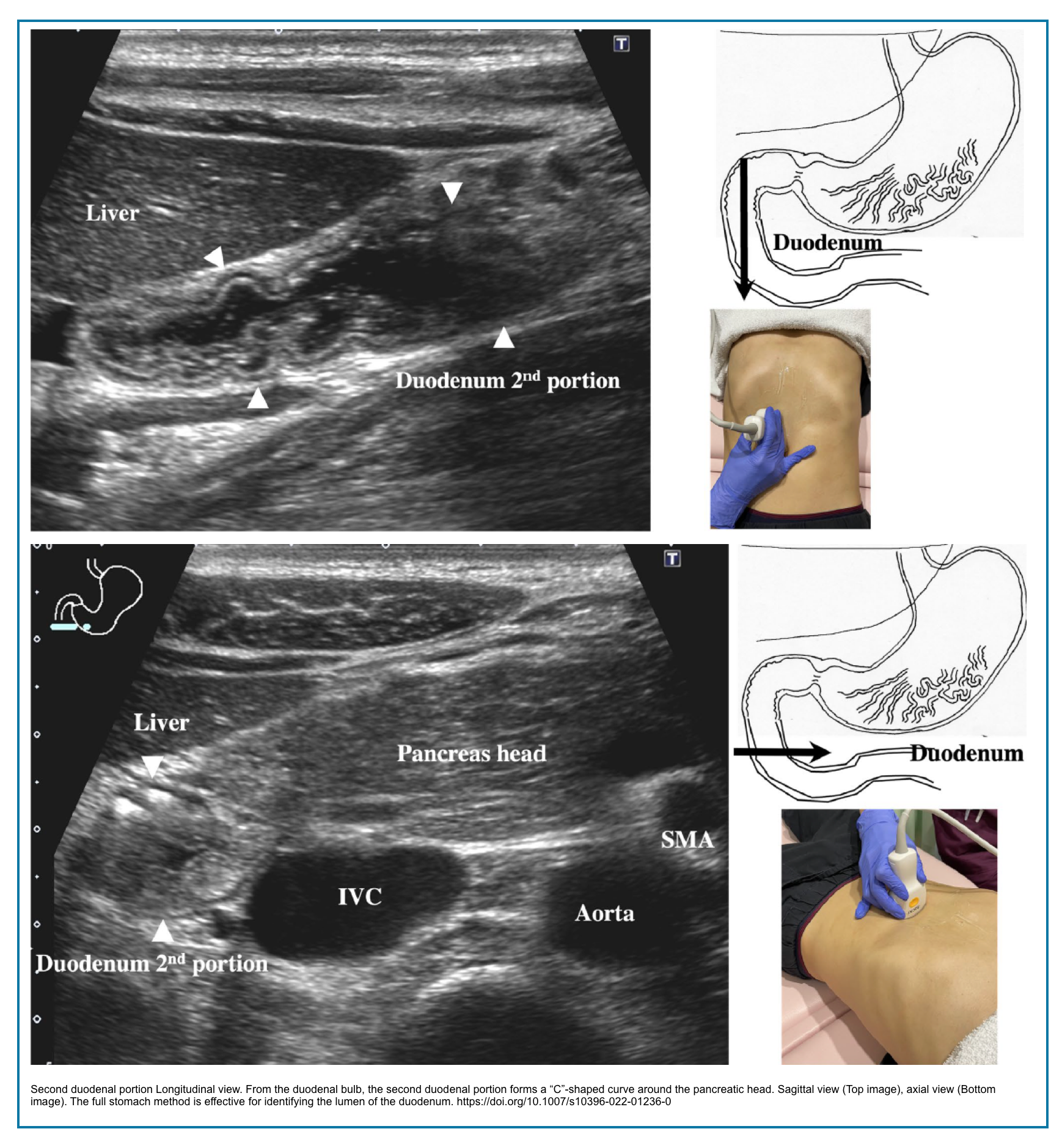
- Intraperitoneal, except for 2nd-4th portions of duodenum, which are retroperitoneal.
- 📍Retroperitoneal structures have a more fixed position and are easy to locate (Right below figure).
- Intraluminal extensions/folds valvulae conniventes, increase surface area for absorption
- Normal measurement of small bowel caliber is < 3 cm.
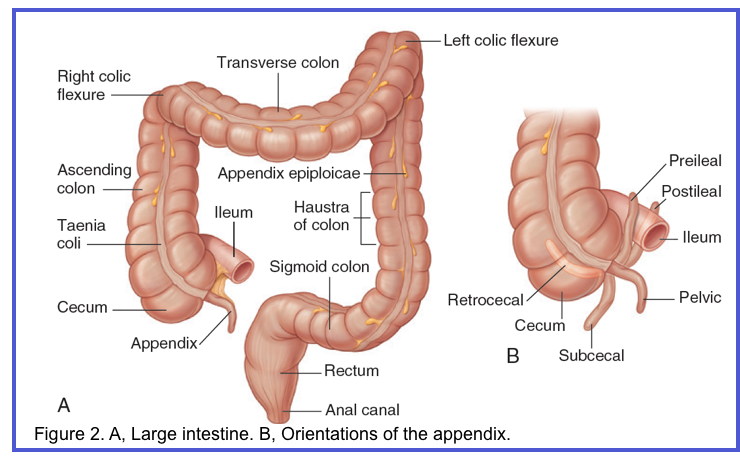
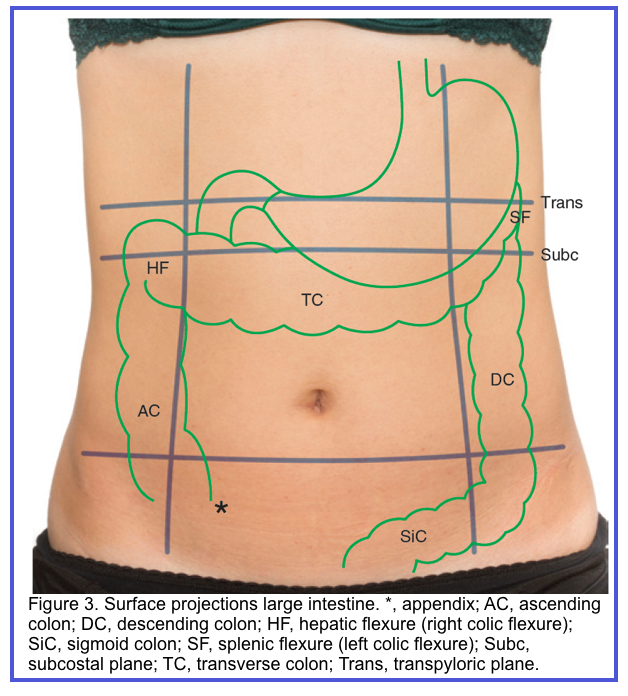
◾️Large bowel
- Between the small bowel and the anus
- ~ 1.5 meters in length
- Peripherally located in the abdomen
- Contain feces and gas
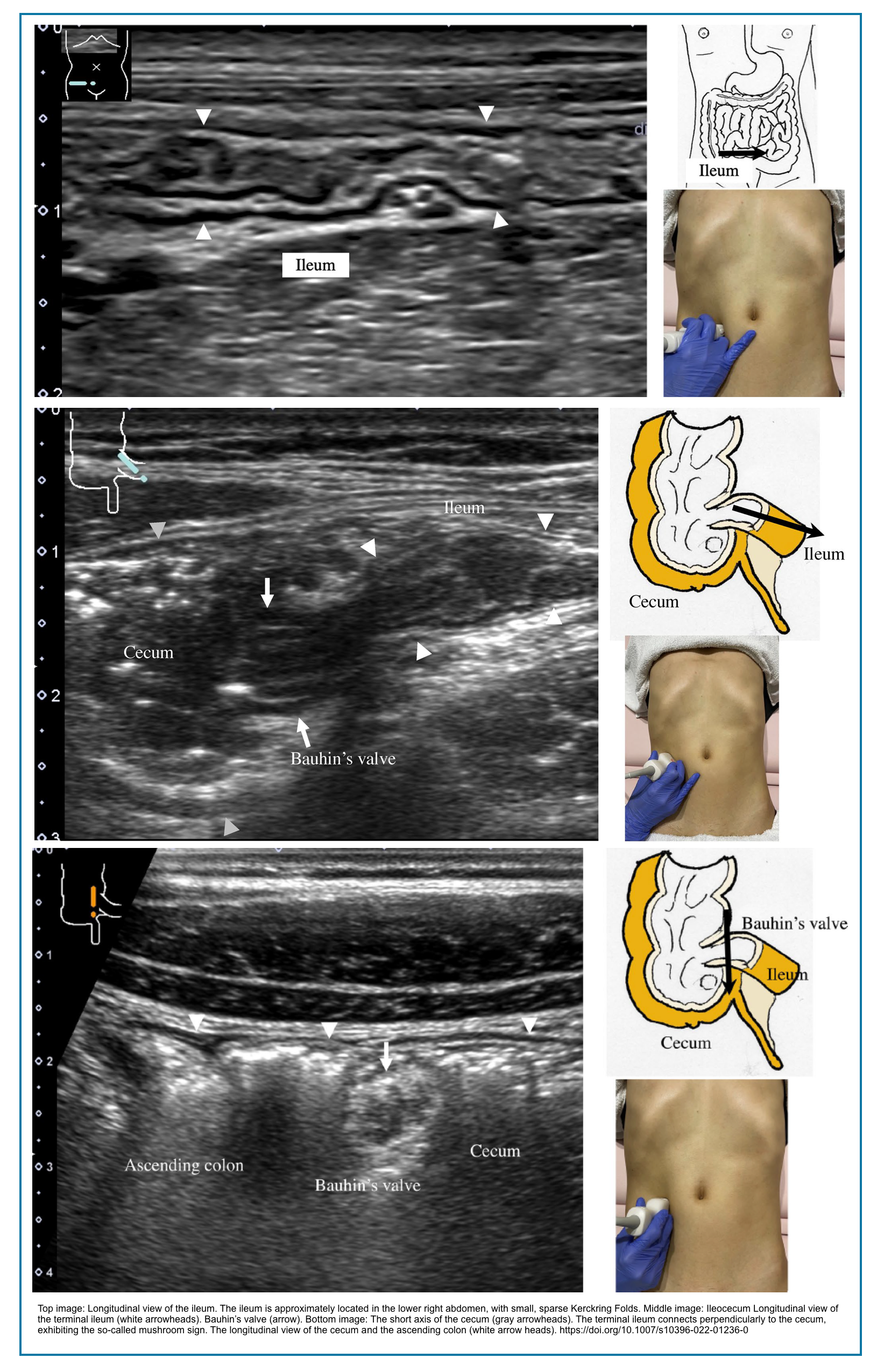
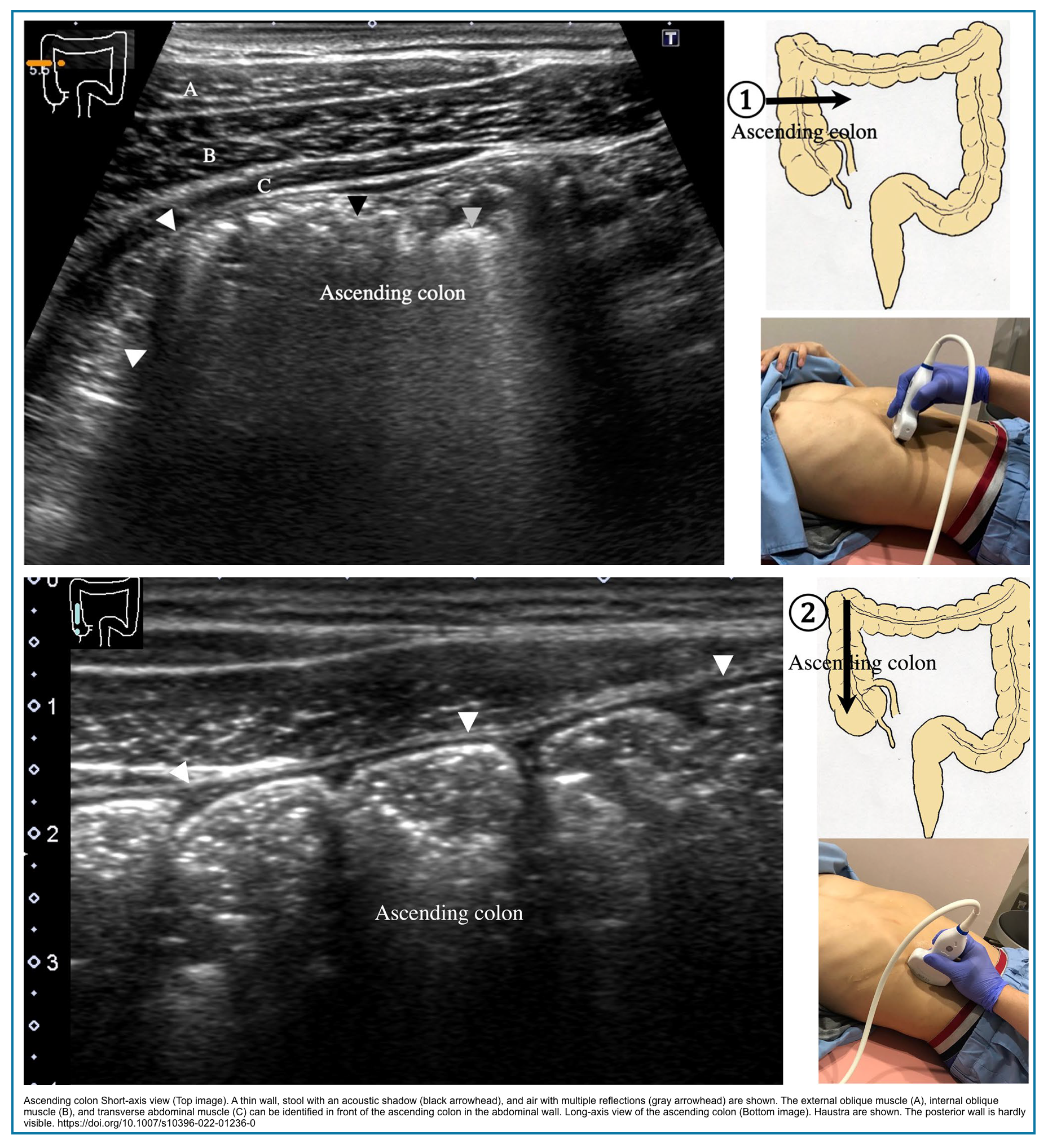
- Cecum and colon identified by haustral pattern.
- Haustra are seen as prominent curvilinear echogenic arcs with posterior reverberation
- Cecum identified by a curvilinear arc of hyperechogenicity (representing feces and gas) in the right lower quadrant, blind-ending caudally
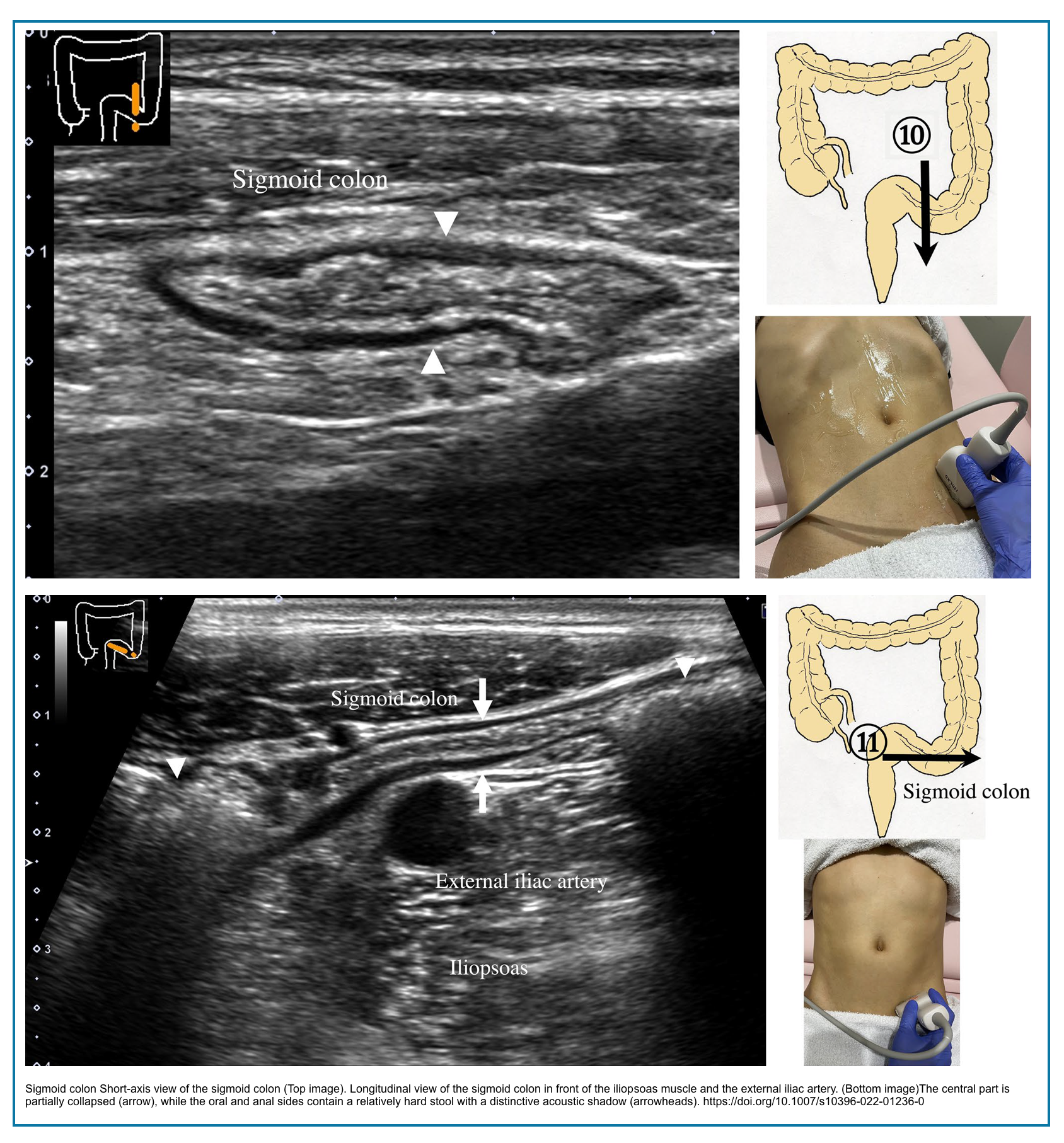
- Cecum and appendix, transverse colon, and rectosigmoid are intraperitoneal
- Ascending colon, descending colon, and middle-to-distal rectum are retroperitoneal.
- Normal caliber of large bowel:
- Cecum < 9 cm
- Transverse colon < 6 cm
◾️Peristalsis
- Refers to the coordinated rhythmic contractions of the bowel wall generated by the muscularis externa and regulated by neural and myogenic control systems, including the interstitial cells of Cajal. On real-time ultrasonography, peristalsis is readily assessed without the need for oral contrast agents.
- Small bowel exhibits active, rapid peristalsis, while colonic motility is slower with predominantly mixing movements.
- Normal bowel loops demonstrate appropriate peristaltic activity for their segment. Diminished or absent peristalsis suggests underlying pathology such as inflammation, ischemia, or obstruction, while hyperperistalsis may be observed in early mechanical obstruction or infectious enteritis.
- Real-time ultrasound offers a unique advantage over CT and MRI by enabling direct dynamic evaluation of bowel motility.
Scanning Technique
◾️Examination of the GI tract is performed after scanning the abdominal solid viscera by using a curvilinear probe.
◾️Probe selection
- Curvilinear probe (1–8 MHz):
- Provides a panoramic overview and orientation to abdominal anatomy
- Allows deeper penetration for obese patients and deeper bowel segments (rectum, retroperitoneal colon)
- Used initially to identify major landmarks and gross abnormalities
- Linear probe (5–12 MHz):
- Offers high-resolution visualization of bowel wall layers
- Enables precise measurement of wall thickness and assessment of stratification
- Essential for evaluating superficial bowel loops and mesenteric fat
- Should be used after a curvilinear overview for detailed interrogation
- Limitations:
- Curvilinear probe lacks sufficient resolution to distinguish the five wall layers
- Linear probe has limited depth penetration (typically <4–6 cm), inadequate for deep or obese patients
◾️B-mode optimization
- 🛠️Technical settings:
- Imaging depth: 8 cm or less (instead of the default 15 cm for liver)
- Focus point positioned just below the target bowel loop
- Lower gain setting preferred to visualize thin intestinal walls
- Narrower dynamic range facilitates identification of wall layers
- Harmonic imaging should be activated when available (improves delineation of wall layers)
- Create a preset button named “Intestine” or “Bowel” for rapid adjustment
- Advantages:
- Optimized settings improve visualization of thin bowel wall layers
- Harmonic imaging reduces artifacts and enhances wall contrast
- Limitations:
- Default abdominal settings often obscure fine bowel wall detail
- Suboptimal settings may lead to false-negative or false-positive findings
◾️GI Tract scanning
- First, the abdominal US probe is used to get an overview before switching to a mid-range to high-frequency probe for a detailed examination.
Then use a linear probe for a more detailed examination of the GI tract. - Start with “Large bowel” scanning *.
- Cecum: Located in the right iliac fossa. Recognizable by its typical content of air and fecal material, as well as its relationship with the narrower ileal loop. This ileal loop usually contains more fluid and particulate content and exhibits noticeable peristalsis. Longitudinal view of the large bowel identifies haustration more easily.
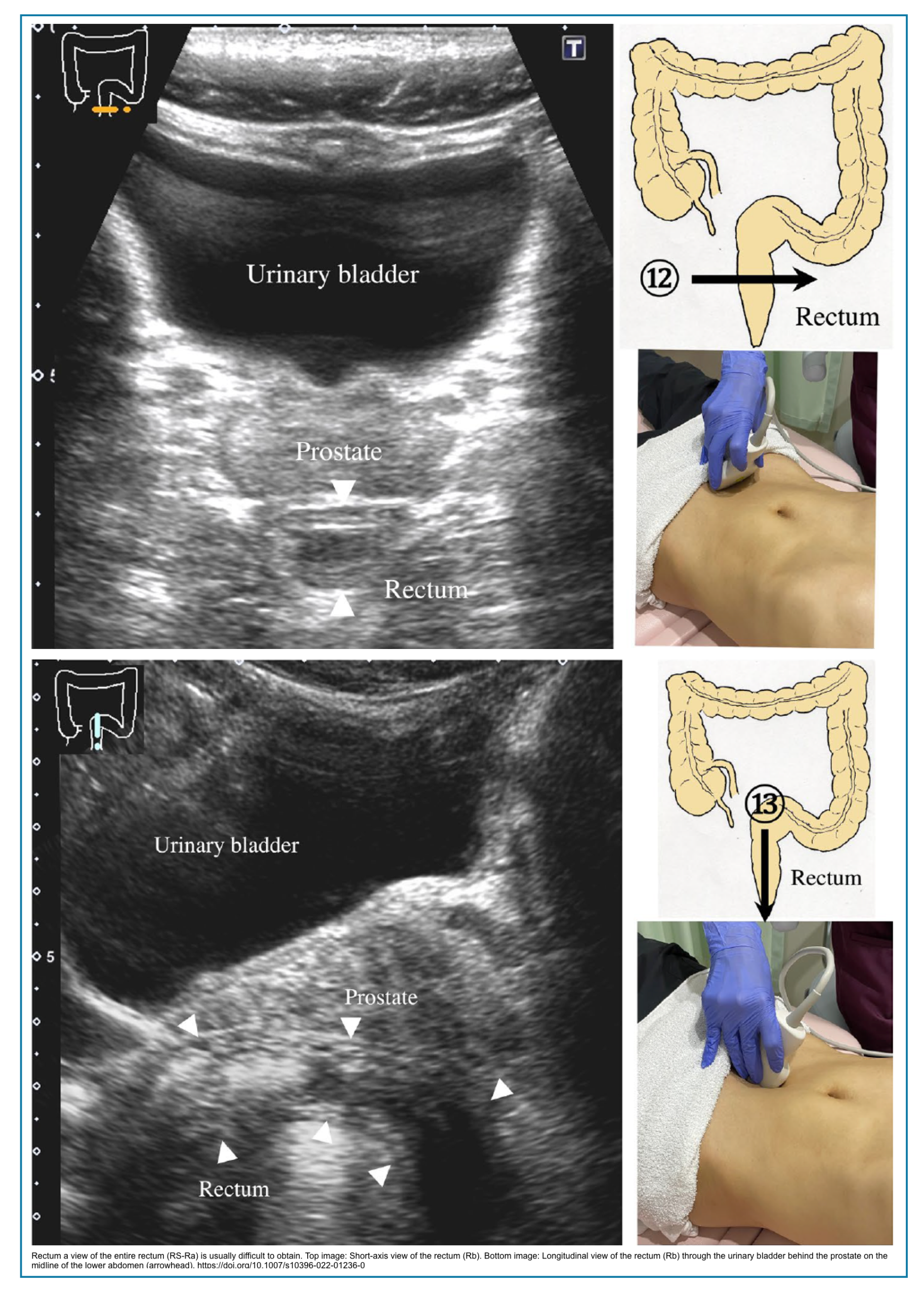
- Rest of the colon: Then, assess the colon systematically by performing a sweep along the entire path of the colon down to the sigmoid colon and rectum in the pelvis. The rectum can be visualized with a full bladder, which serves as an acoustic window.
- Small bowel: Identify the terminal ileum and trace it as far as possible proximally. For the exploration of jejunal and ileal loops, parallel transverse scans are recommended, moving across the abdomen from one side to the other in a craniocaudal direction, encompassing the entire abdominal area.
◾️Slow graded compression
- Normal bowel is readily compressible, shows peristaltic activity, and dispels intraluminal gas.
- Slow graded compression is useful for the following reasons:
- The compression helps displace endoluminal gas.
- This can push away overlying bowel segments with gas or intra-abdominal fat and, in this way, enable the examiner to reach deeper with high-frequency probes, such as in the pelvis.
- Assess the compressibility of the examined loop.
- This is a crucial observation in contrast to abnormal bowel, which is usually thick-walled, rigid, demonstrates reduced peristalsis, and remains in a relatively fixed position.
- Identify tender points that might disclose underlying pathology.
- This technique also allows for the demonstration of localized peritonism, which increases the index of suspicion for underlying focal pathology.
- The compression helps displace endoluminal gas.
◾️Doppler assessment
- Provides additional information regarding the vascularity of the bowel wall and adjacent fat; however, this technique has a limited sensitivity due to artifact.
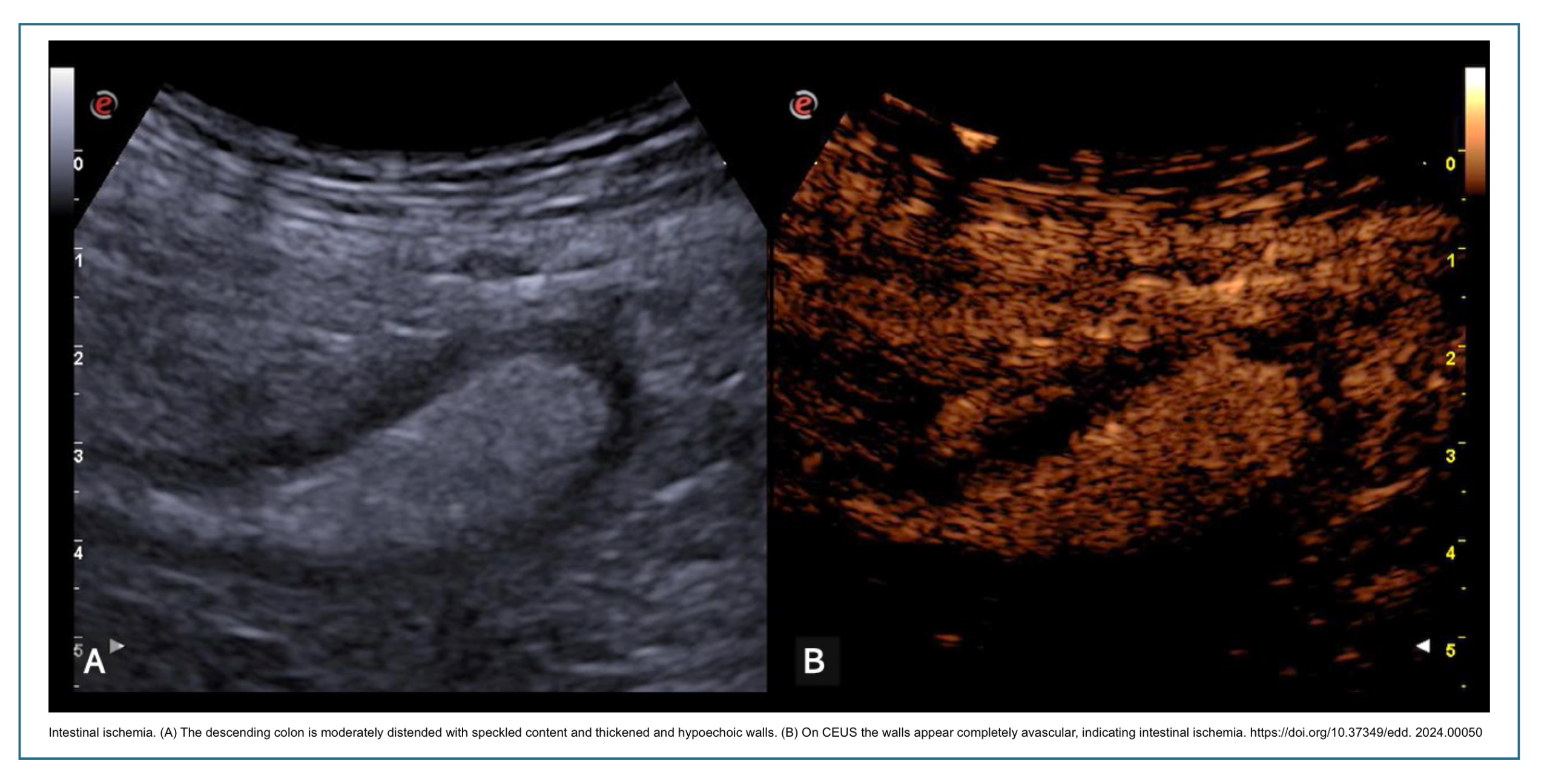
- Increased vascularity is typically seen in infectious or inflammatory thickening, and the absence of flow can potentially indicate bowel ischemia. These findings require correlation with the underlying clinical context and baseline ultrasound images.
- 🛠️Technical settings:
- Color or Power Doppler should be used to evaluate bowel wall vascularity.
- Velocity scale set low: 2–5 cm/s (to detect slow-velocity flow in small mural vessels).
- Wall filter adjusted to the lowest setting.
- Color gain turned up until flash artifacts appear, then reduced slightly until they disappear.
- Pulse repetition frequency (PRF): low setting to maximize sensitivity.
- 🧒Patient cooperation:
- Patient should hold breath during image acquisition to minimize respiratory motion.
- Breath-holding reduces flash artifacts and improves Doppler signal detection.
- Advantages:
- Provides a semiquantitative assessment of bowel wall inflammation.
- Hyperemia correlates with active inflammation (infectious or inflammatory).
- Absence of flow in thickened bowel suggests ischemia (specific, though not highly sensitive).
- Helps differentiate between inflammatory and fibrotic strictures (increased vs. absent flow).
- Can be repeated serially to monitor treatment response without radiation.
- Limitations:
- Limited sensitivity for slow or low-volume flow, particularly in deep bowel loops (>4 cm depth)
- Flash artifacts from peristalsis and patient movement degrade image quality.
- Operator-dependent for both acquisition and interpretation.
- High body mass index reduces depth penetration and signal detection.
- Normal bowel wall rarely demonstrates detectable Doppler signals, limiting baseline comparison.
- Cannot detect capillary flow (only larger intramural vessels).
Correlated US findings of bowel wall histology
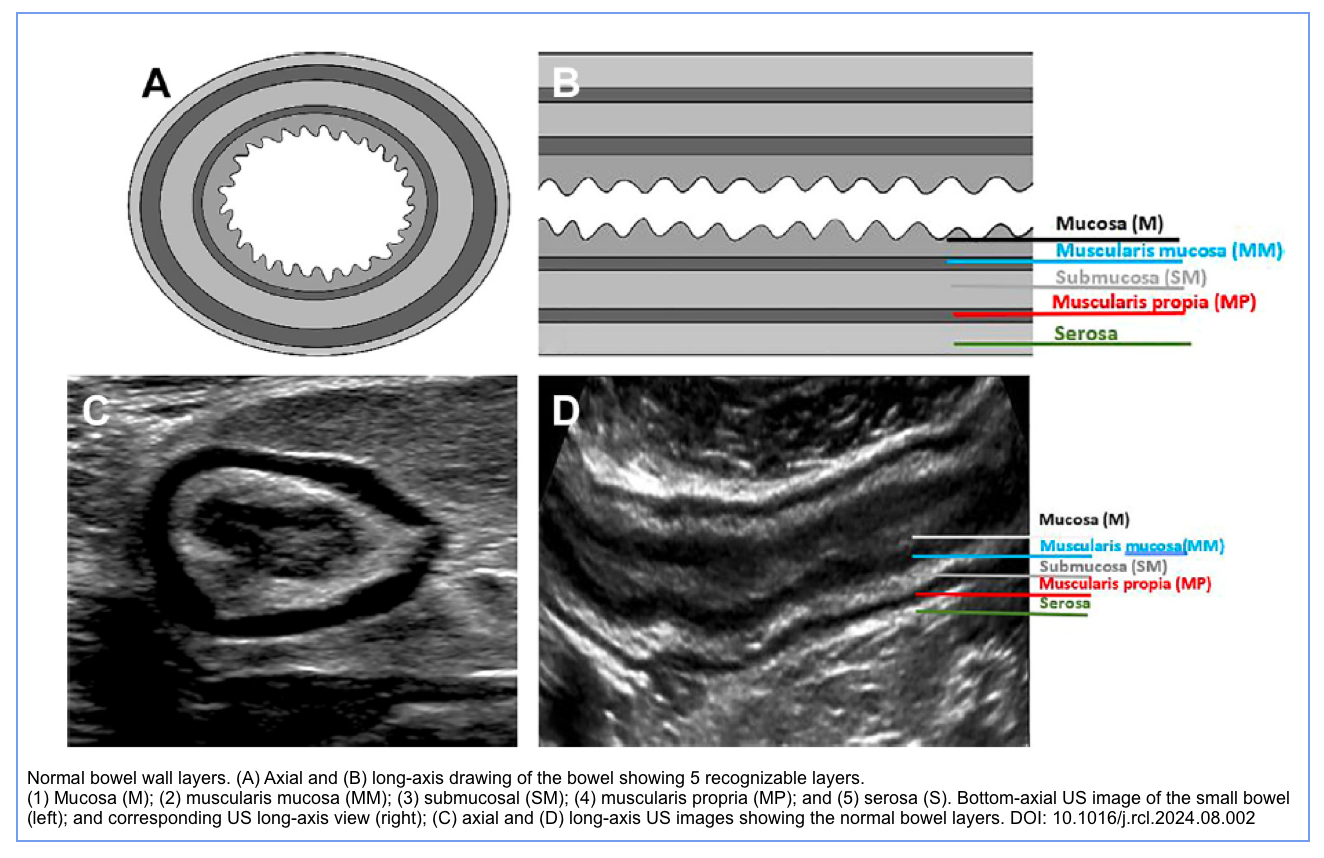
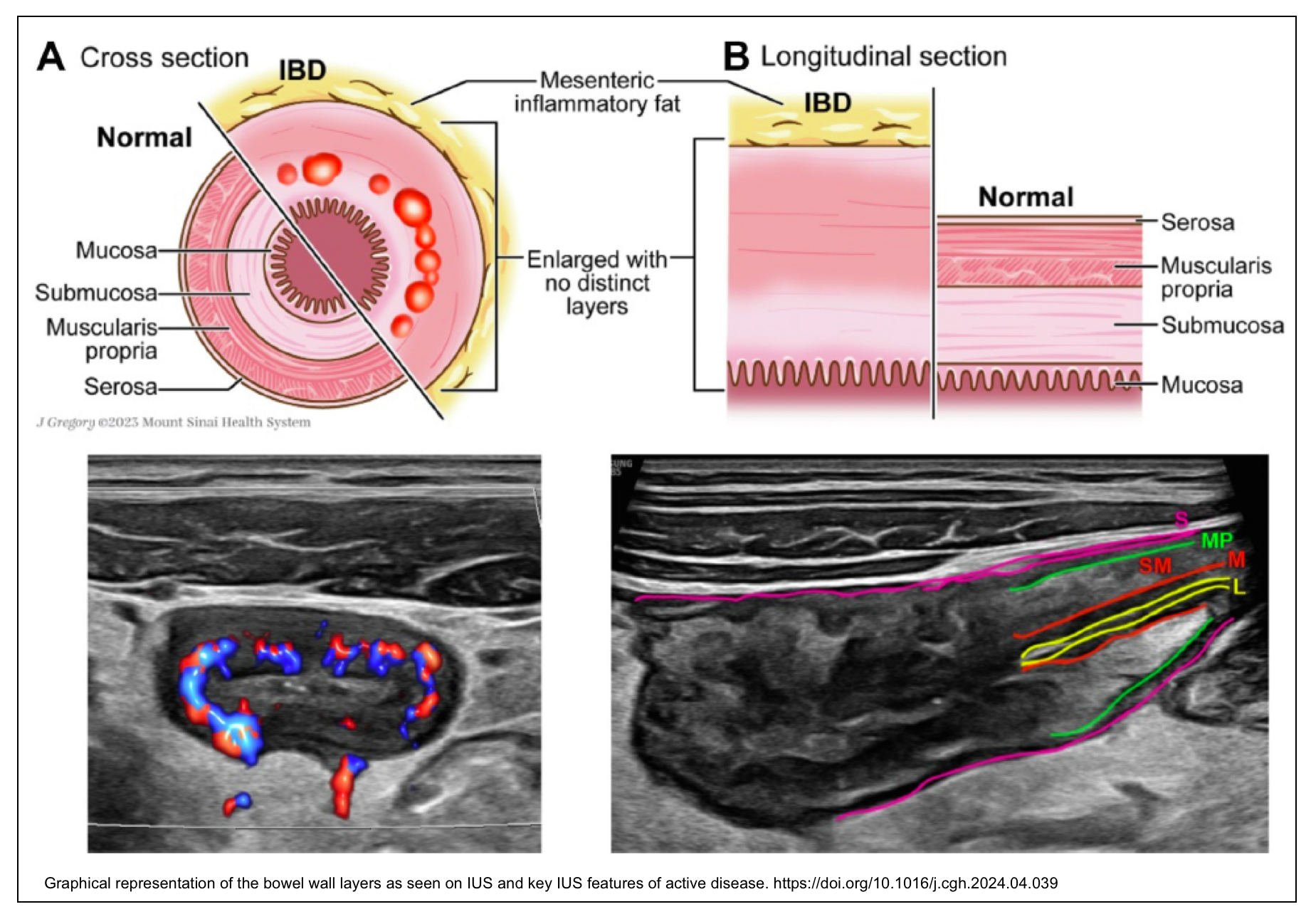
◾️The bowel wall throughout the GI tract has uniform general histology, comprised of 4 layers
- Mucosa
- Functions for absorption and secretion
- Composed of epithelium and loose connective tissue
- Lamina propria
- Muscularis mucosa (deep layer of mucosa)
- Submucosa (This is the thickest layer)
- The submucosa contains vessels, nerves, and fat and is hyperechoic due to abundant loose connective tissue.
- Muscularis externa
- The muscularis is hypoechoic (due to muscular tissue), and the outer black layer is easy to identify. The muscular layer responsible for peristalsis. Contains Auerbach plexus
- Serosa
- The epithelial lining is continuous with the peritoneum. The serosa or visceral peritoneum is the thin but tough outer hyperechoic layer, which usually blends with the hyperechoic fatty tissue of mesentery and omentum, surrounding the bowel.
- If there is intraperitoneal fluid, the hyperechoic serosa (arrow) can be separately identified, as in these ileal loops.
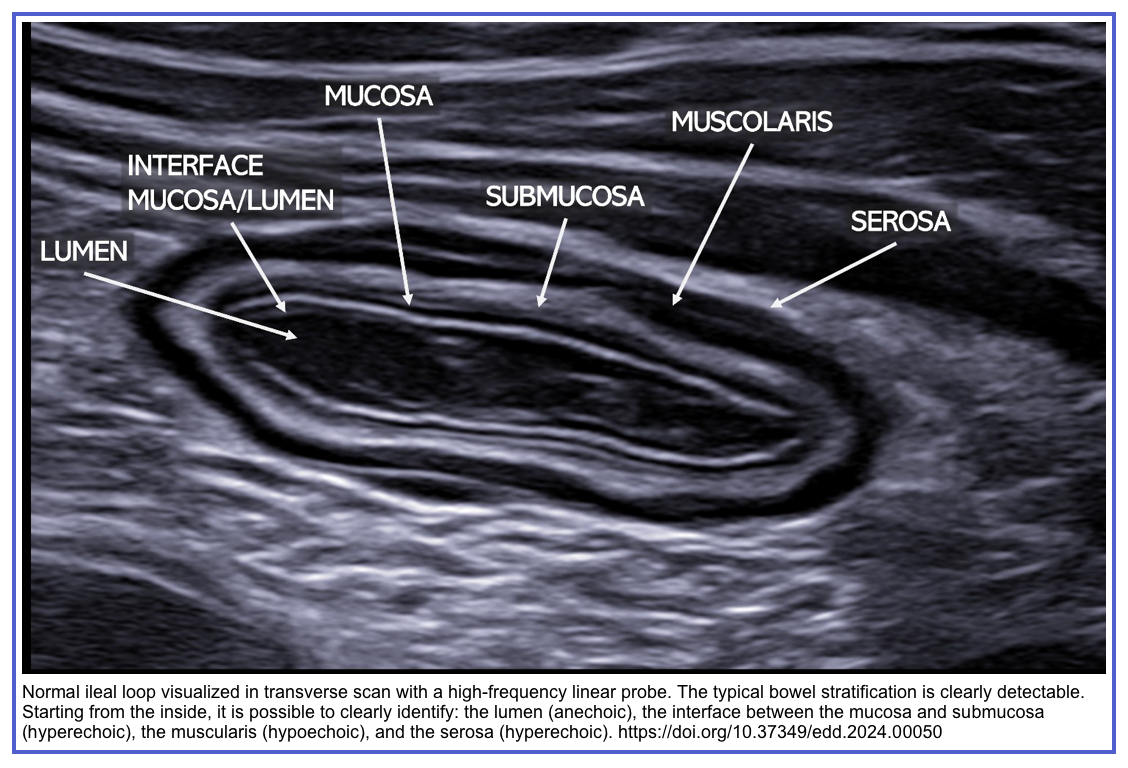
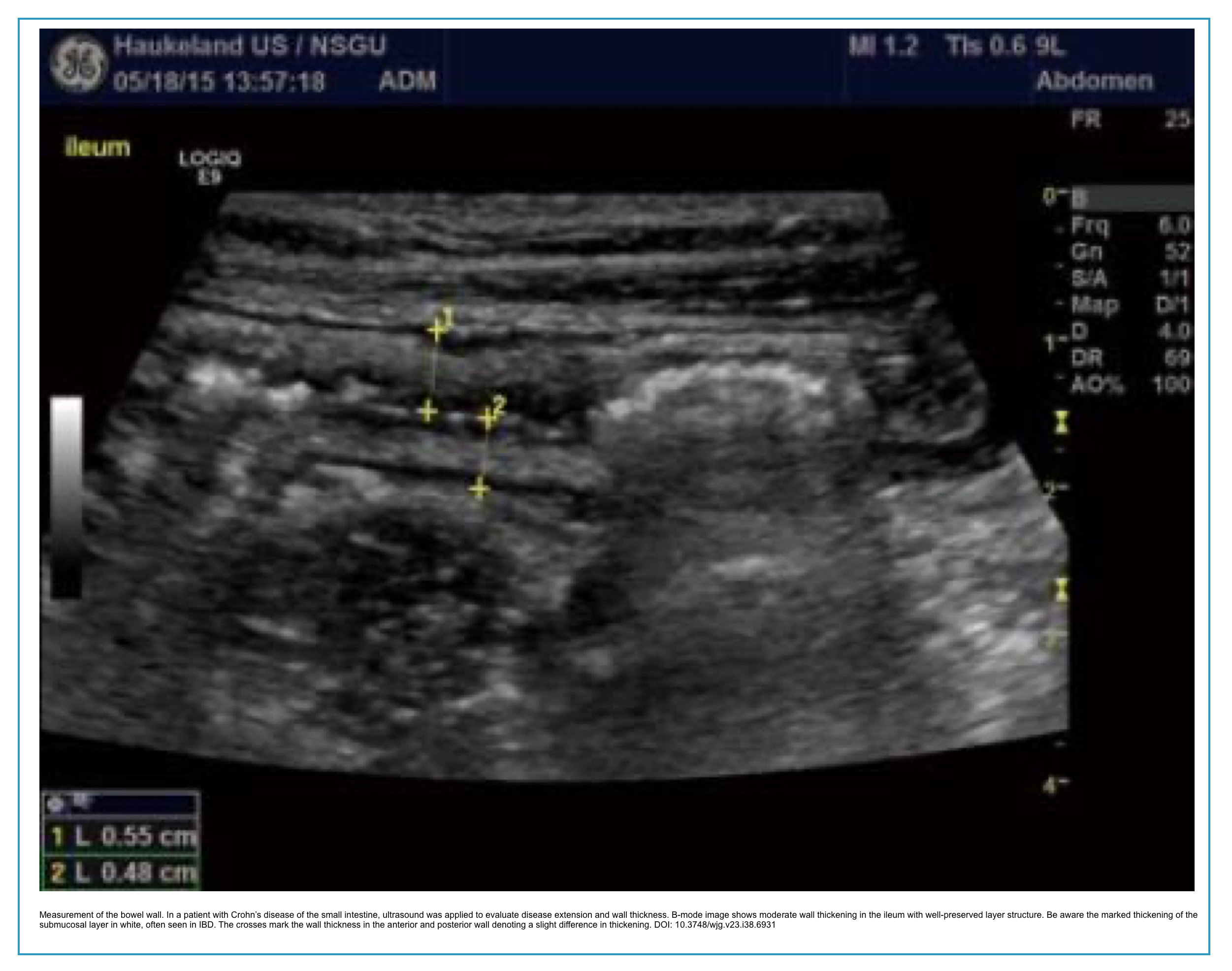
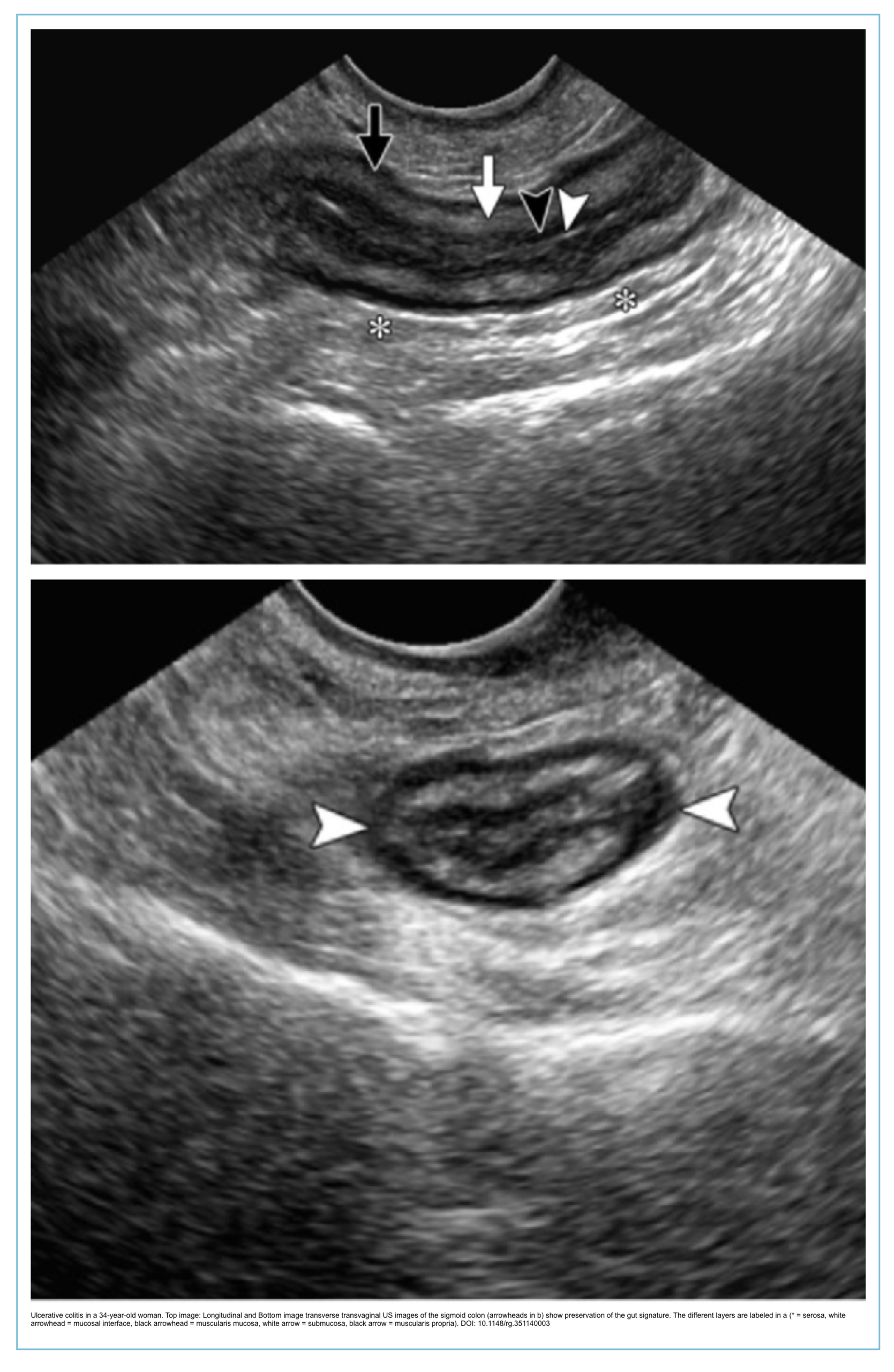
◾️Ultrasound appearance of the bowel wall
- Stratified appearance of bowel wall on histology is depicted by 5 distinct layers on ultrasound as alternating echogenic/sonolucent (hypoechoic) appearance (gut signature).
- 🔎Transducer frequency and layer visualization
- Curvilinear probe (3–5 MHz): Typically shows only 2–3 layers (inner hyperechoic submucosa + outer hypoechoic muscularis propria)
- Linear probe (7–12 MHz): All 5 layers readily distinguished
- Linear probe (12–18 MHz): Optimal for detailed layer analysis but limited depth penetration
- ✅ Normal wall thickness values by segments:
- Small intestine: ≤ 3 mm
- Colon: ≤ 4 mm
- Stomach: ≤ 5–6 mm
- Rectum: ≤ 7 mm
💡Normal bowel wall thickness is less than 3 mm, with an average maximum single-wall thickness of 3–5 mm depending on the degree of distension.
💡The number of visible layers depends on transducer frequency and proximity to the gut wall. With a curvilinear probe (5 MHz), the transverse section of the bowel demonstrates a stratified target-like appearance with an inner hyperechoic layer (submucosa) and a hypoechoic outer rim (muscularis propria).
✅Using a linear transducer (12–18 MHz), all five distinct layers can be readily appreciated; on axial imaging, a pattern of concentric rings with alternating hyperechoic and hypoechoic bands is seen.
- 💡Clinical pearl – loss of stratification
- Preservation of the 5-layer signature suggests a benign or inflammatory etiology
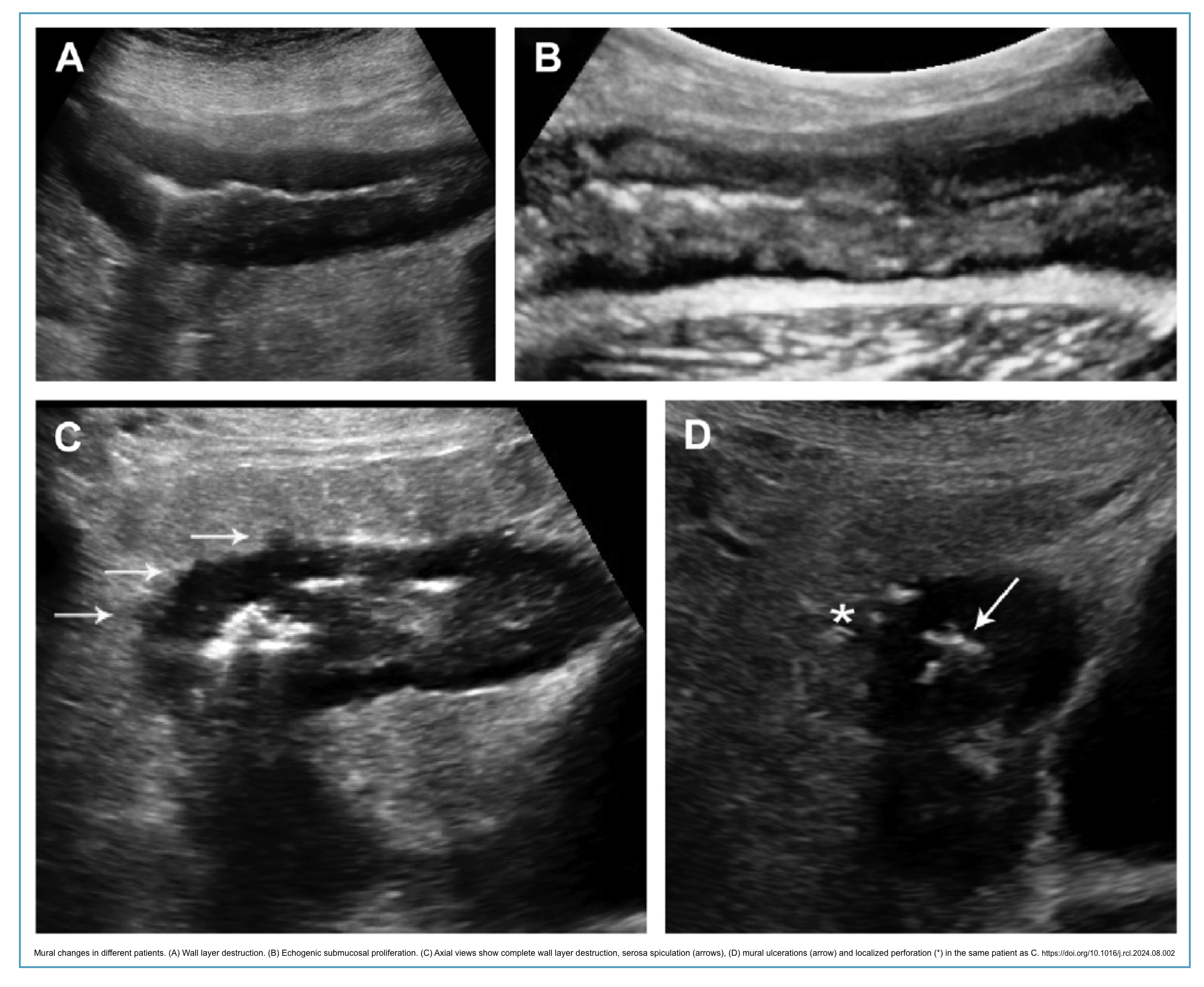
- Disruption or loss of stratification raises suspicion of severe transmural inflammation (e.g., active Crohn’s disease) or malignancy.
- Anisotropy artifact warning
- Bowel wall layers appear most distinct when the ultrasound beam is perpendicular to the wall.
- Oblique angles may artificially blur or obliterate layer distinction.
💡Features of small bowel loops include their central location, presence of valvulae conniventes, and active peristalsis.
💡In contrast, the colon demonstrates a heterogeneous haustral pattern associated with a prominent linear arc of gas and posterior reverberation artifact.
Key Sonographic Parameters for Diagnosing GI disease
- Physiological gut signature refers to a lumen that is normal for this segment, a wall structure with characteristic layering, well-defined wall thickness, and normal peristalsis.
- Pathological gut signature is characterized by changes in the normal appearance of the lumen, wall thickness, and/or peristalsis/pliability.
Click to expand/collapse table
| Parameter | Considerations |
|---|---|
| Wall thickness | Measured perpendicular from lumen-mucosa interface to serosa. Normal: small bowel ≤3 mm, colon ≤4 mm. Thickening is nonspecific (inflammatory, infectious, ischemic, neoplastic). |
| Wall layer structure (layering) | Preservation of 5-layer signature suggests benign/inflammatory etiology. Loss of stratification suggests severe transmural inflammation (e.g., active Crohn’s) or malignancy. |
| Wall stiffness (pliability) | Assessed with graded compression. Normal bowel is compressible. Rigid, non-compressible bowel suggests fibrosis, malignancy, or severe inflammation. |
| Peristalsis | Assessed in real-time. Diminished/absent: inflammation, ischemia, obstruction. Hyperperistalsis: early obstruction, infectious enteritis. |
| Lumen and contents | Assess luminal diameter (constricted or distended). Contents: anechoic fluid, echogenic chyme, hyperechoic feces, air, foreign bodies, bezoars. |
| Vascularity (blood flow signal) | Color/Power Doppler. Hyperemia: active inflammation. Absent flow: ischemia (specific, not highly sensitive). Normal bowel rarely shows detectable flow. |
| Location/distribution | Diffuse vs. localized. Segmental vs. continuous. Anatomic location helps narrow differential diagnosis (e.g., terminal ileum: Crohn’s). |
| Internal and external delineation | Clarity of bowel wall and serosal margins. Poor delineation suggests transmural disease extension or adjacent inflammation. |
| Findings outside the wall | Assess adjacent fat: inflamed hyperechoic fat (useful clue). Look for enlarged lymph nodes, fluid collections, abscesses, fistulas, creeping fat. |
Wall thickness
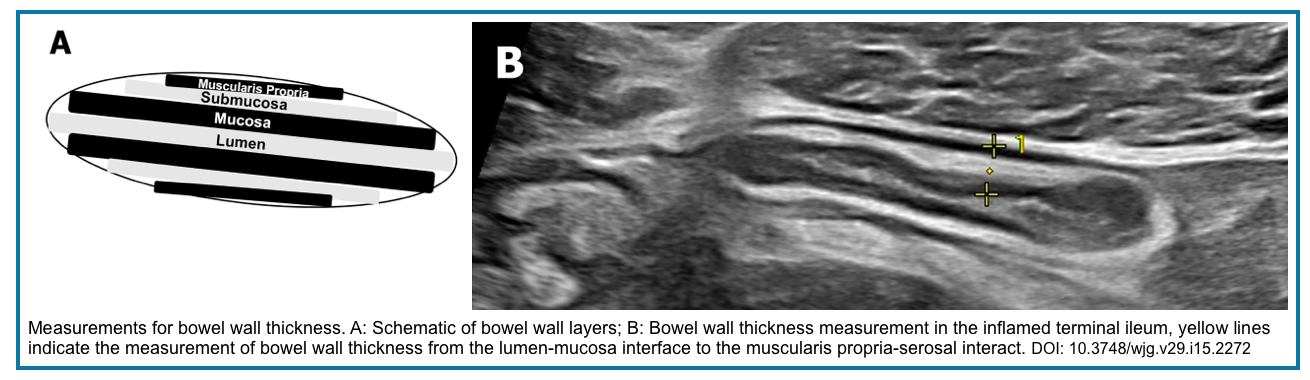
- Measurement technique:
- Measured perpendicularly from the lumen-mucosa interface to the serosa (White To White).
- Use a high-frequency linear probe (5–12 MHz) for accurate measurement.
- Perform measurement under mild compression with transducer perpendicular to bowel wall to avoid tangential overestimation.
- Normal values 👉 Above
- Clinical significance of bowel wall thickening (BWT):
- Thickening is the most common and reliable sign of bowel disease, but it is nonspecific.
- Symmetric thickening: suggests an inflammatory or infectious etiology.
- Asymmetric thickening: raises suspicion for neoplasm (e.g., lymphoma, adenocarcinoma).
- The degree of thickening does not reliably differentiate between benign and malignant causes.
- Differential diagnosis of BWT:
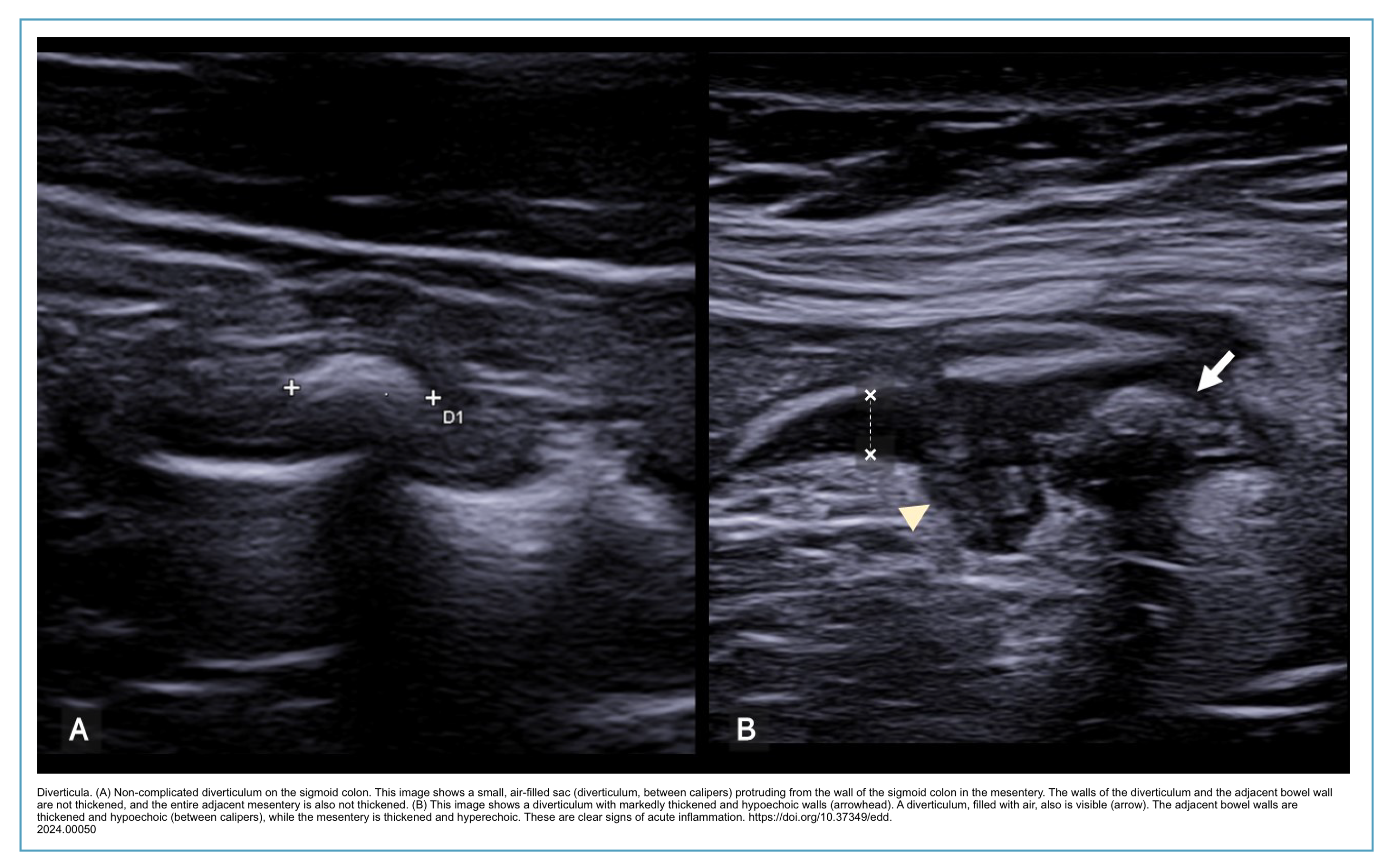
- Inflammatory: Crohn’s disease, ulcerative colitis, infectious enteritis, diverticulitis
- Ischemic: bowel ischemia, ischemic colitis
- Neoplastic: adenocarcinoma, lymphoma, GIST
- Other: intramural hemorrhage, edema, radiation enteritis
Wall layer structure (layering)
- Normal appearance (STRATFIED APPEARANCE)
- Five alternating hyperechoic and hypoechoic layers (gut signature), explained above.
- Best visualized with a high-frequency linear probe (7–12 MHz).
- 🛠️Assessment technique:
- Scan perpendicular to bowel wall to avoid anisotropy artifact.
- Use minimal compression to preserve layer distinction.
- Optimize focus point at the level of the bowel wall.
- Clinical implication
- Preserved stratification:
- Suggests a benign or inflammatory etiology.
- Typically seen in: ulcerative colitis (mucosal involvement), mild Crohn’s disease, infectious enteritis, diverticulitis.
- Loss of stratification:
- Indicates severe transmural inflammation or malignancy.
- Typically seen in: Active Crohn’s disease (transmural), lymphoma, adenocarcinoma, severe ischemia.
- Associated with a higher risk of complications (fistulas, abscesses).
- Preserved stratification:
- 💡Clinical pearl:
- Preservation of the 5-layer signature is a reassuring sign that argues against malignancy.
- Complete loss of stratification in a thickened bowel loop warrants further investigation (cross-sectional imaging or endoscopy).
Wall stiffness (pliability)
- 🛠️Assessment technique:
- Evaluated using graded compression with the ultrasound probe
- Apply gradual pressure while following respiratory movements
- Compare the compressibility of the abnormal segment to the adjacent normal bowel
- ✅Normal findings:
- Normal bowel is readily compressible
- Bowel walls approximate, or the lumen collapses completely under gentle pressure
- Intraluminal gas is displaced, improving visualization of deeper structures
- ⚠️Abnormal findings (rigid, non-compressible):
- Inflammatory: Active Crohn’s disease, severe diverticulitis, phlegmon
- Fibrotic: Chronic fibrotic stricture (preserved layering, no hyperemia)
- Neoplastic: Adenocarcinoma, lymphoma, GIST
- Ischemic: Non-viable bowel, transmural infarction
- 💡Clinical significance:
- Loss of compressibility is a key distinguishing feature between normal and abnormal bowel.
- Helps differentiate between functional (dynamic) ileus and mechanical obstruction.
- Rigid, fixed loops with loss of peristalsis suggest transmural disease
- Fibrotic strictures typically show preserved layering but increased stiffness compared to inflammatory strictures
- Limitations:
- Limited efficacy in obese patients (increased abdominal wall thickness)
- Patient discomfort may limit compression over tender areas
- Overly aggressive compression may distort wall architecture

💡Clinical Pearl
📋 Table. Differentiating Paralytic Ileus from Mechanical Obstruction (Click to expand)
| Feature | Paralytic Ileus | Mechanical Obstruction |
|---|---|---|
| Peristalsis | Absent | Hyperperistalsis (early) → absent (late) |
| Transition point | Absent | Present |
| Colon appearance | Filled with fluid, gas, stool | Empty or collapsed distal to obstruction |
| Wall thickness | Normal or thinned | May be thickened at obstruction site |
| Compressibility | Decreased (fluid-filled, no peristalsis) | Normal proximal loops; non-compressible at transition |
Peristalsis
- Assessment technique:
- Evaluated in real-time using B-mode ultrasound
- Observe a segment of bowel for 10–20 seconds to assess contraction frequency and amplitude
- Document findings with cine clips for serial comparison
- Normal findings:
- Small bowel: active, coordinated, progressive contractions
- Large bowel: slower, less frequent, predominantly mixing movements
- Normal peristalsis helps displace intraluminal gas and contents
📋 Abnormal Peristalsis Findings (Click to expand)
| Finding | Clinical Association |
|---|---|
| Diminished or absent | Inflammation (active Crohn’s), ischemia, paralytic ileus, advanced obstruction, infiltrative diseases |
| Hyperperistalsis | Early mechanical obstruction, infectious enteritis, malabsorption (celiac disease) |
| To-and-fro movement | Partial obstruction (pendular movements without net propulsion) |
| Aperistalsis (fixed loop) | Severe transmural inflammation, fibrosis, malignancy |
- Clinical significance:
- Real-time ultrasound offers a unique advantage over CT and MRI for motility assessment
- Diminished peristalsis is an indicator of unhealthy bowel
- Absent peristalsis in a dilated, fluid-filled loop suggests paralytic ileus (📽️ videlow below).
- 💡PEARL: Sonographic criteria for small bowel obstruction:
- 3 or more dilated loops of bowels
- Bowel dilation >2.5cm
- Alternating (bidirectional) peristalsis (luminal contents cannot keep moving forward due to obstruction)
- 💡PEARL: Sonographic criteria for small bowel obstruction:
- Hyperperistalsis proximal to a transition point suggests mechanical obstruction (more on this: 🔗here).
- Limitations:
- Subjective assessment (operator-dependent)
- Fasting reduces baseline small bowel motility
- Deep or gas-obscured loops may be difficult to assess
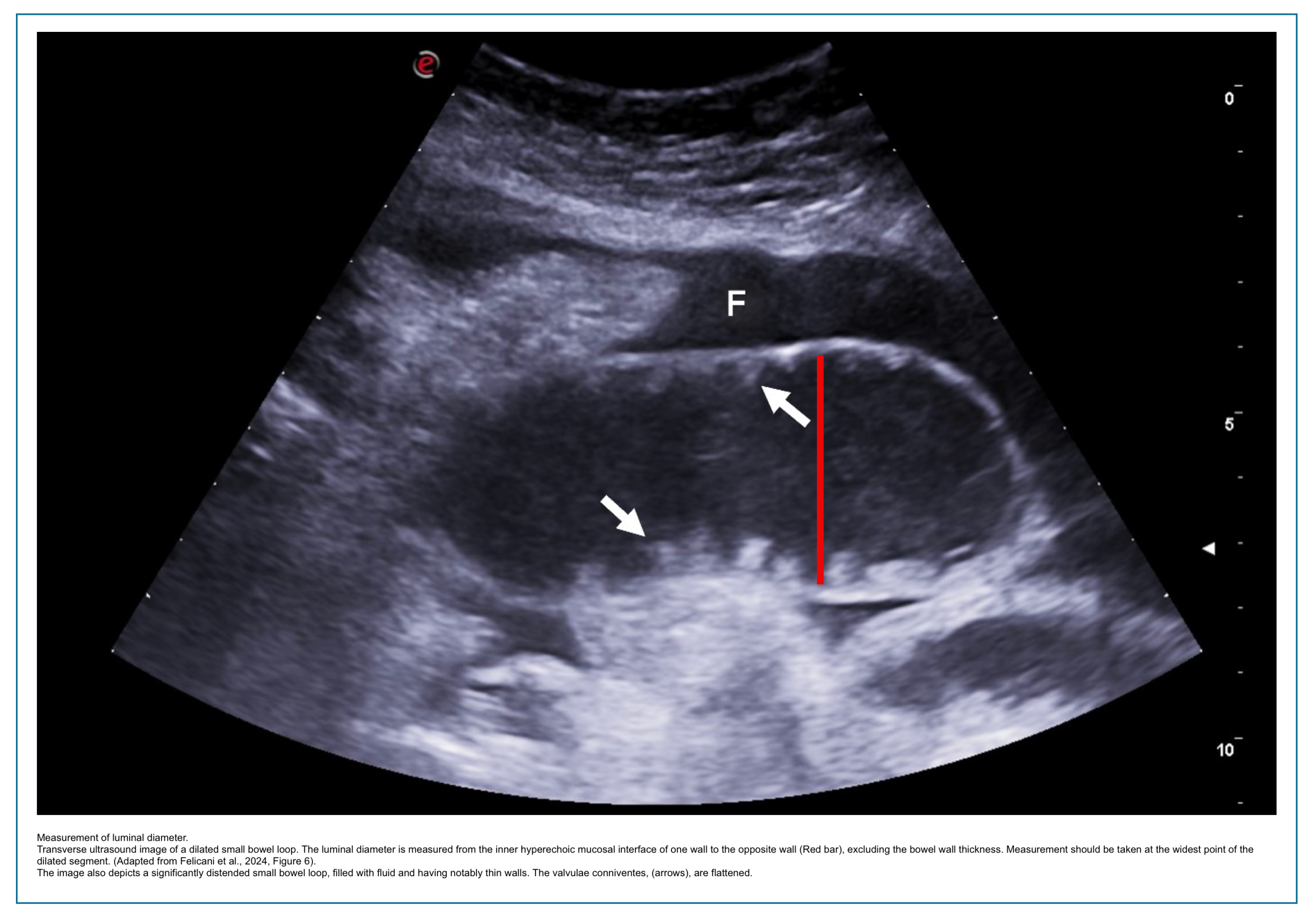
Luminial diameter and contents
- 🛠️Assessment technique:
- Luminal contents: Assess contents using B-mode ultrasound with graded compression
- Note the presence, quantity, and echogenicity of intraluminal material
- Luminal diameter: Assess in transverse and longitudinal planes:
- Luminal diameter is measured from inner wall to inner wall (from the mucosal interface of one wall to the mucosal interface of the opposite wall) in a transverse or axial plane of the bowel loop.
- Luminal contents: Assess contents using B-mode ultrasound with graded compression
📋 Table. Measurement Technique for Luminal Diameter (Click to expand)
| Step | Description |
|---|---|
| 1 | Identify the bowel loop in transverse (axial) plane |
| 2 | Measure from inner wall to inner wall (mucosa-to-mucosa) |
| 3 | Avoid including the bowel wall thickness in the measurement |
| 4 | Perform measurement under mild compression to displace intraluminal gas |
| 5 | Take measurement at the widest point of the dilated segment |
| 6 | For obstructions, measure proximal to the transition point |
- ✅Normal findings:
- Luminal contents:
- Small bowel: fluid and particulate content (hypoechoic/anechoic with some echogenic particles)
- Colon: feces and gas (hyperechoic with posterior shadowing and reverberation artifacts)
- Luminal diameter
- Normal small bowel caliber: < 3 cm
- Normal colonic caliber: cecum < 9 cm, transverse colon < 6 cm
- Luminal contents:
📋 Table. Luminal Diameter Measurement by Ultrasound (Click to expand)
| Bowel Segment | Normal Diameter | Abnormal (Dilated) |
|---|---|---|
| Small bowel | < 2.5 cm (25 mm) | > 2.5–3.0 cm |
| Cecum | < 9 cm | > 9 cm |
| Transverse colon | < 6 cm | > 6 cm |
| Colon (general) | < 5 cm | > 5 cm |
| Appendix | < 6–7 mm (outer diameter) | > 6–7 mm |
📋 Table. Abnormal Luminal Diameter Findings (Click to expand)
| Finding | Clinical Association | ||||
|---|---|---|---|---|---|
| Dilatation (small bowel >3 cm, colon >6 cm) | Obstruction (mechanical or paralytic ileus), toxic megacolon, chronic pseudo-obstruction | ||||
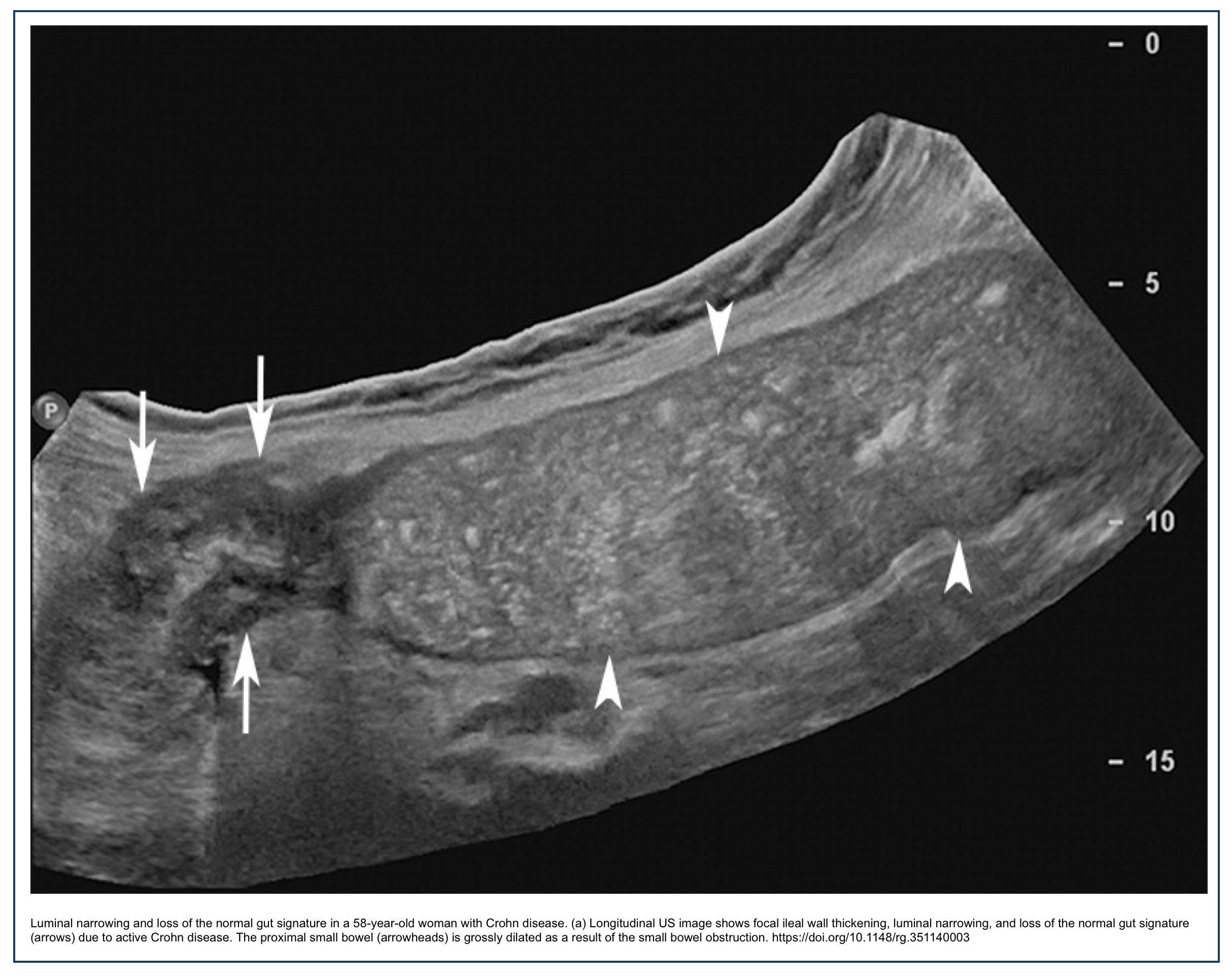
| Luminal narrowing (<10 mm at stricture site) | Stricture (inflammatory or fibrotic), malignancy, external compression |
| Content | Ultrasound Appearance | Clinical Association |
|---|---|---|
| Excessive anechoic fluid | Anechoic, mobile | Small bowel obstruction, SIBO, malabsorption, infectious enteritis |
| Echogenic chyme/ingesta | Mixed echogenicity | Normal postprandial state, delayed gastric emptying |
| Hyperechoic feces/scybala | Hyperechoic with posterior shadowing | Constipation, fecal impaction |
| Air (intraluminal) | Hyperechoic with reverberation artifact | Normal colonic finding; excessive suggests SIBO or ileus |
| Foreign bodies / bezoars | Hyperechoic arc-like surface with posterior shadowing; possible twinkling artifact on Doppler | Ingested objects, phytobezoars, trichobezoars |
- Clinical significance:
- Dilated small bowel loops with fluid content and hyperperistalsis suggest early mechanical obstruction
- Dilated loops with absent peristalsis suggest paralytic ileus
- Fecal loading in the rectum with posterior shadowing suggests constipation
- Bezoars may demonstrate a “twinkling artifact” on color Doppler, helping differentiate them from fecal material
Vascularity (blood flow signal)
- 🛠️Assessment technique:
- Use Color or Power Doppler with low velocity scale (2–5 cm/s)
- Wall filter set to lowest setting
- Color gain adjusted until flash artifacts appear, then reduced slightly
- Power Doppler may be more sensitive than Color Doppler for detecting slow flow in small mural vessels
- Patient holds breath during acquisition to minimize motion artifact
- Assess both the bowel wall and the adjacent mesenteric fat
- Normal findings:
- Normal bowel wall rarely demonstrates detectable Doppler signals
- Absence of flow in healthy, non-thickened bowel is expected
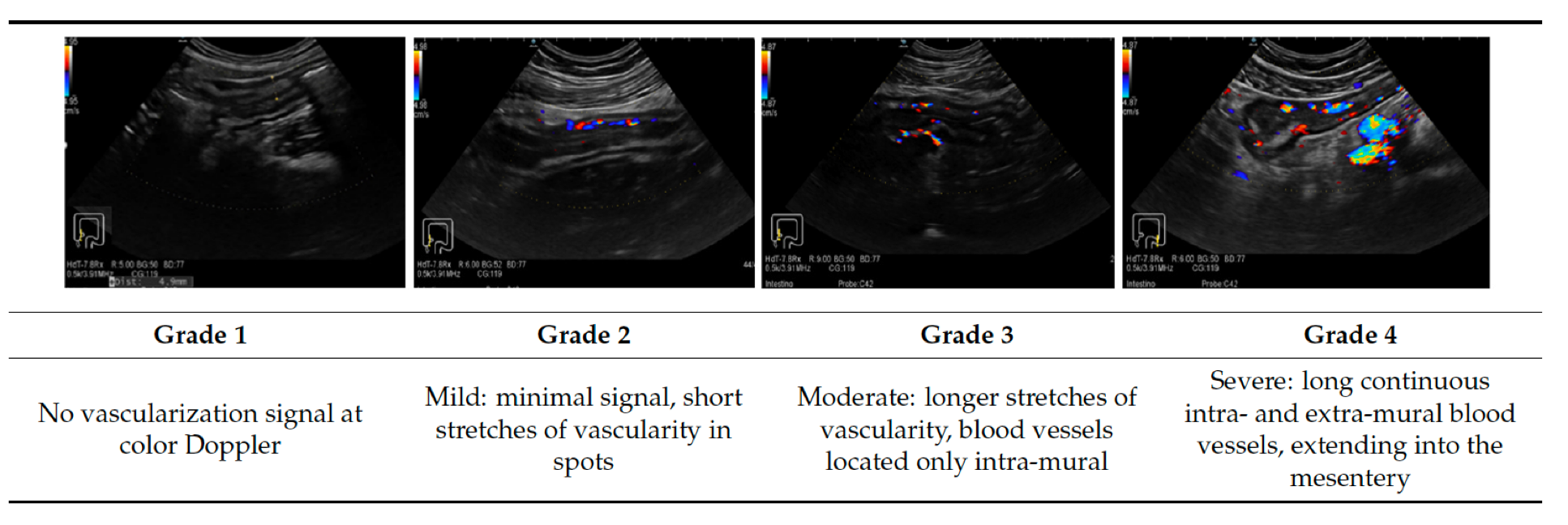
- Limberg Score
- Vascularity score for MUC: 0 = absent; 1 = mild (spotty); 2 = moderate (long stretches within wall); 3 = severe (stretches extending into mesentery)
Click to expand/collapse table
| Finding | Ultrasound Appearance | Clinical Association |
|---|---|---|
| Increased vascularity (hyperemia) | Multiple color signals in wall/submucosa | Active inflammation (Crohn’s disease, ulcerative colitis, infectious enteritis, diverticulitis) |
| Absent flow | No detectable color signals in thickened bowel wall | Ischemia (specific, though not highly sensitive), fibrotic stricture |
| Preserved but normal flow | Scant or no signals | Chronic inactive disease, fibrotic stricture |
- 💡Clinical significance:
- Hyperemia correlates with active inflammation and neovascularization
- Useful for monitoring treatment response (decreased vascularity suggests response to anti-inflammatory therapy)
- Differentiates inflammatory from fibrotic strictures (increased vs. absent flow)
- Absence of flow in thickened bowel suggests ischemia, especially in the correct clinical context
- Limitations:
- Limited sensitivity for slow or low-volume flow, particularly in deep bowel loops (>4 cm)
- Flash artifacts from peristalsis and respiratory motion degrade image quality
- High body mass index reduces depth penetration and signal detection
- Cannot detect capillary flow (only larger intramural vessels)
Location/distribution
- Assessment technique:
- Systematically scan all four quadrants using both curvilinear and linear probes
- Trace abnormal bowel loops to document the length and pattern of involvement
- Note the anatomic segment(s) affected (e.g., terminal ileum, ascending colon, sigmoid)
- Document whether involvement is single or multifocal
- Normal findings:
- Small bowel: centrally located, jejunum in the left upper/mid abdomen, ileum in the right lower abdomen
- Colon: peripherally located (picture-frame distribution)
- Retroperitoneal segments (ascending colon, descending colon, rectum) have fixed positions
📋 Abnormal Distribution Patterns (Click to expand)
| Pattern | Description | Clinical Association |
|---|---|---|
| Segmental | Single, discrete segment of involvement | Crohn’s disease (skip lesions), diverticulitis, ischemia, neoplasm |
| Continuous | Long, uninterrupted involvement | Ulcerative colitis (from rectum proximally), infectious colitis |
| Diffuse | Widespread involvement of small or large bowel | Severe enteritis, pan-enteric Crohn’s disease, pseudo-obstruction |
| Skip lesions | Intervening normal bowel between abnormal segments | Crohn’s disease (hallmark feature) |
| Right-sided | Involvement of cecum, ascending colon, terminal ileum | Crohn’s disease, appendicitis, infectious ileocecitis |
| Left-sided | Involvement of descending colon, sigmoid, rectum | Ulcerative colitis, diverticulitis, ischemic colitis |
- Clinical significance:
- Anatomic location helps narrow the differential diagnosis
- Terminal ileum involvement: Crohn’s disease, infectious ileitis, tuberculosis
- Periappendiceal location: appendicitis, Crohn’s disease involving the cecum
- Rectal sparing: Crohn’s disease (suggests against ulcerative colitis)
- Segmental with skip lesions: highly suggestive of Crohn’s disease
- Continuous from rectum proximally: suggestive of ulcerative colitis
Internal and external delineation
- 🛠️Assessment technique:
- Evaluate clarity of the bowel wall layers (internal delineation)
- Assess the serosal margin and its interface with surrounding tissues (external delineation)
- Use a high-frequency linear probe with optimal focus and gain settings
- Compare affected segment to adjacent normal bowel
- ✅Normal findings:
- Internal: Five distinct wall layers clearly visualized (when using a high-frequency probe)
- External: Smooth, well-defined hyperechoic serosal margin
- Clear separation between bowel wall and adjacent mesenteric fat
Click to expand/collapse table
| Finding | Ultrasound Appearance | Clinical Association |
|---|---|---|
| Poor internal delineation | Blurred or obscured wall layers | Severe transmural inflammation (active Crohn’s), edema, malignancy, ischemia |
| Loss of layer distinction | Cannot identify individual layers | Inflammatory mass, phlegmon, advanced malignancy |
| Poor external delineation | Indistinct serosal margin | Transmural disease extension, adjacent inflammation, creeping fat |
| Matted loops | Loss of separation between adjacent bowel loops | Peritoneal carcinomatosis, severe IBD, intra-abdominal adhesions |
- Clinical significance:
- Good internal delineation favors a benign/inflammatory etiology
- Poor internal delineation with loss of stratification raises suspicion for malignancy or severe transmural inflammation
- Poor external delineation suggests disease extension beyond the bowel wall
- Matted, inseparable loops indicate significant intra-abdominal pathology (adhesions, carcinomatosis, active IBD)
- Limitations:
- Deep bowel loops or an obese body habitus reduce visualization quality
- Overlying bowel gas may obscure segments
- Operator-dependent for optimal image acquisition
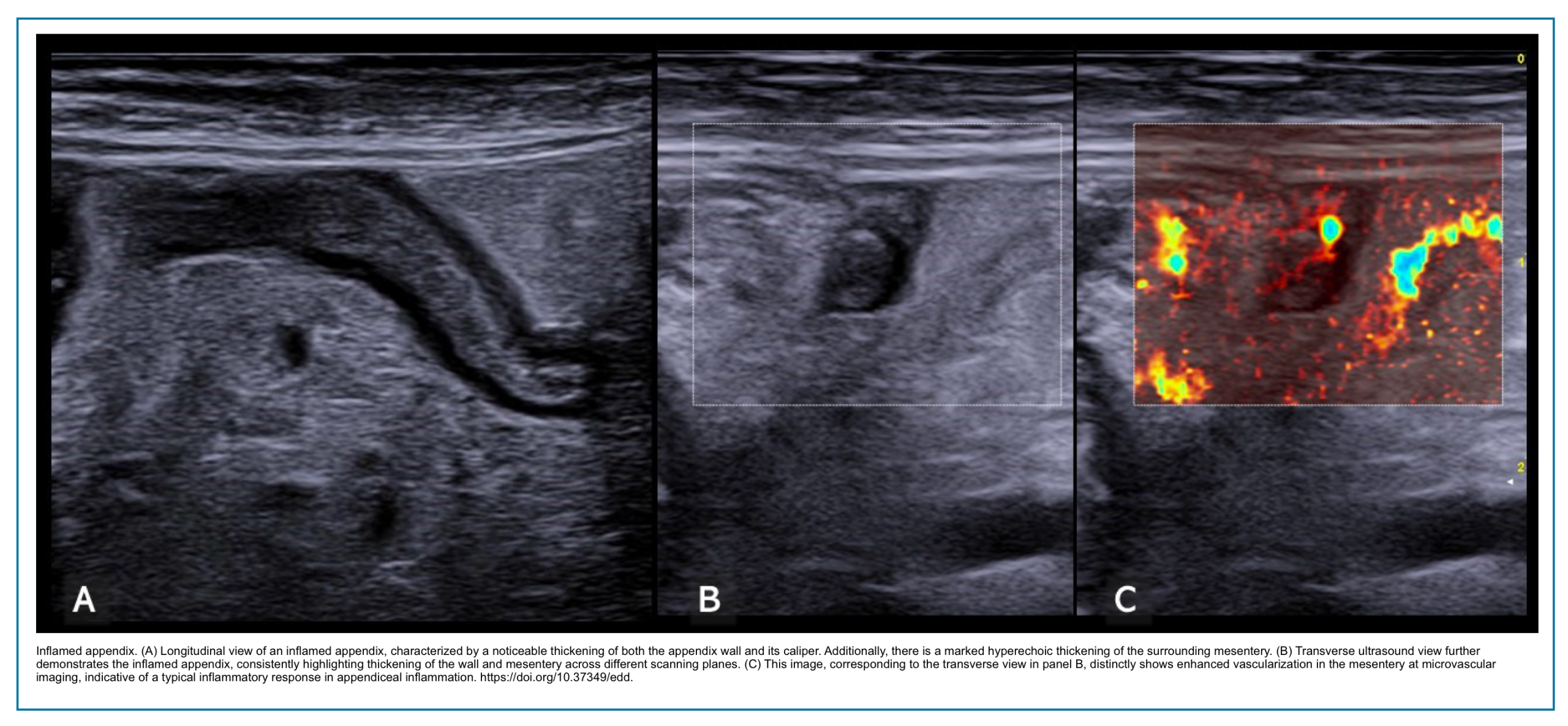
Findings outside the wall
- Assessment technique:
- Evaluate mesenteric fat adjacent to thickened bowel loops
- Assess for lymphadenopathy, fluid collections, and free peritoneal fluid
- Use graded compression to displace overlying bowel gas
- Apply color Doppler to assess the vascularity of extramural lesions
- Normal findings:
- Mesenteric fat: hypoechoic parallel layers, 7–12 mm thick
- Lymph nodes: oval, elongated, hypoechoic; short axis < 4 mm in adults
- No free fluid or collections
📋 Abnormal Findings Outside the Wall (Click to expand)
| Finding | Ultrasound Appearance | Clinical Association |
|---|---|---|
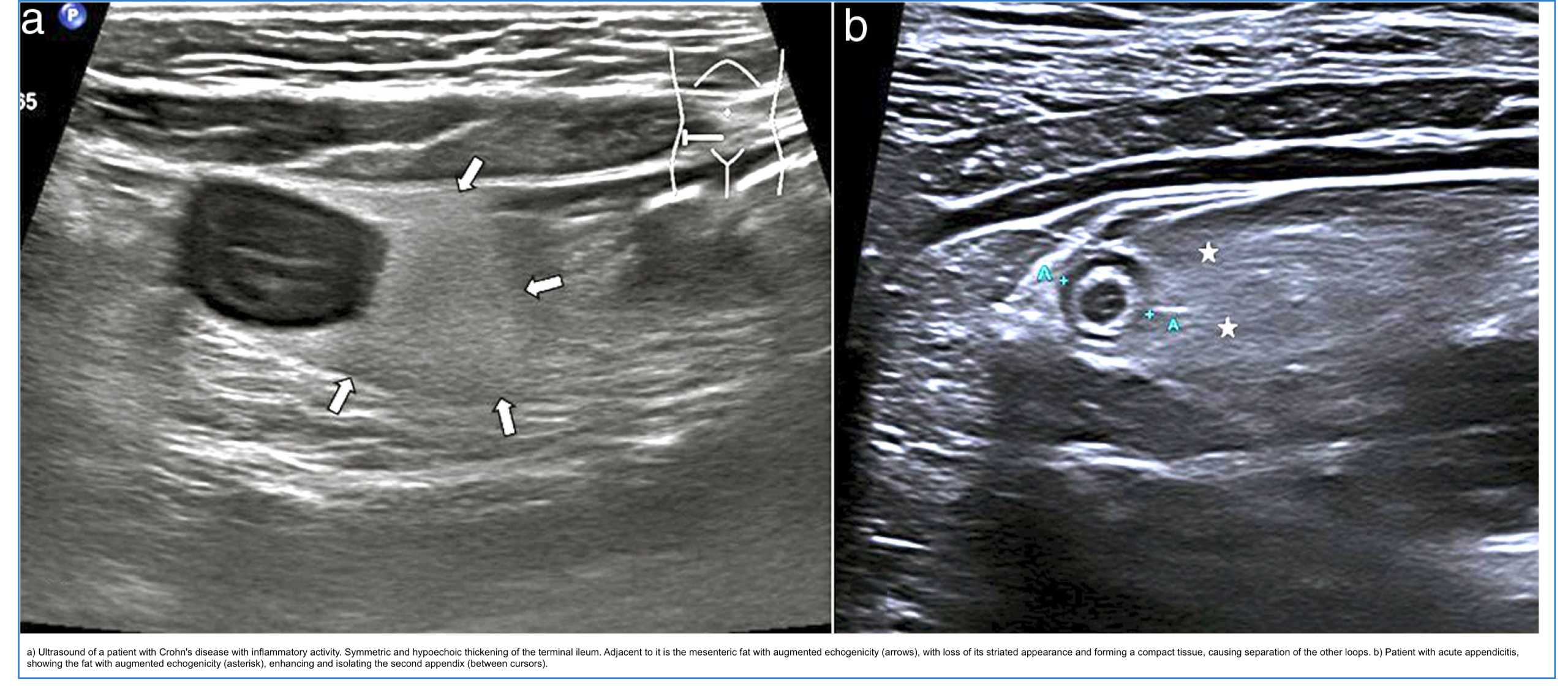
| Inflamed hyperechoic fat | Increased echogenicity of mesenteric/omental fat | Acute diverticulitis, appendicitis, Crohn’s disease (creeping fat) |
| Creeping fat | Echogenic fat extending >50% of bowel circumference, separating loops | Crohn’s disease (specific feature) |
| Enlarged lymph nodes | Short axis >4 mm (adults) or >10 mm (children); may show increased vascularity | Inflammatory bowel disease, infectious enteritis, malignancy |
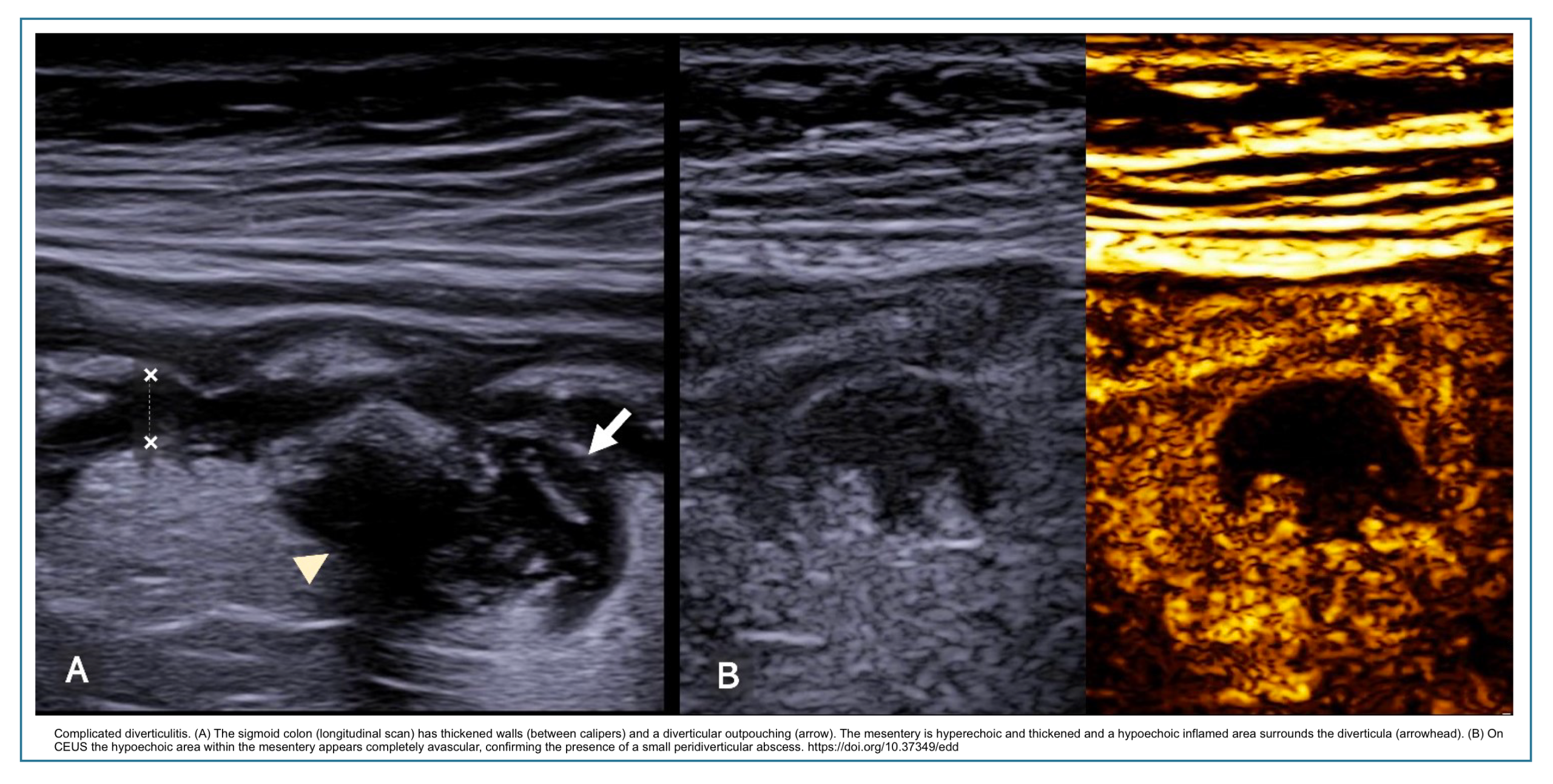
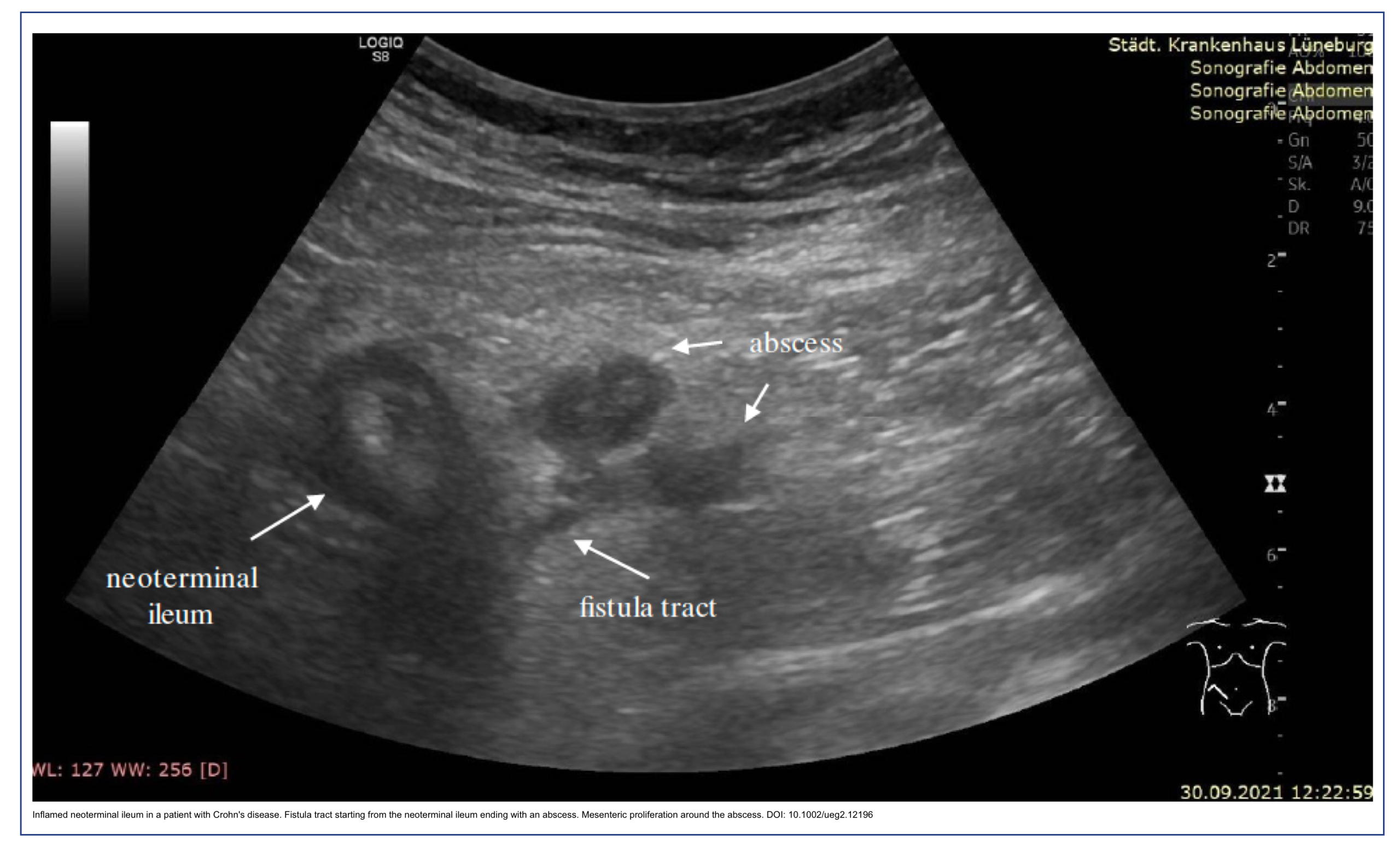
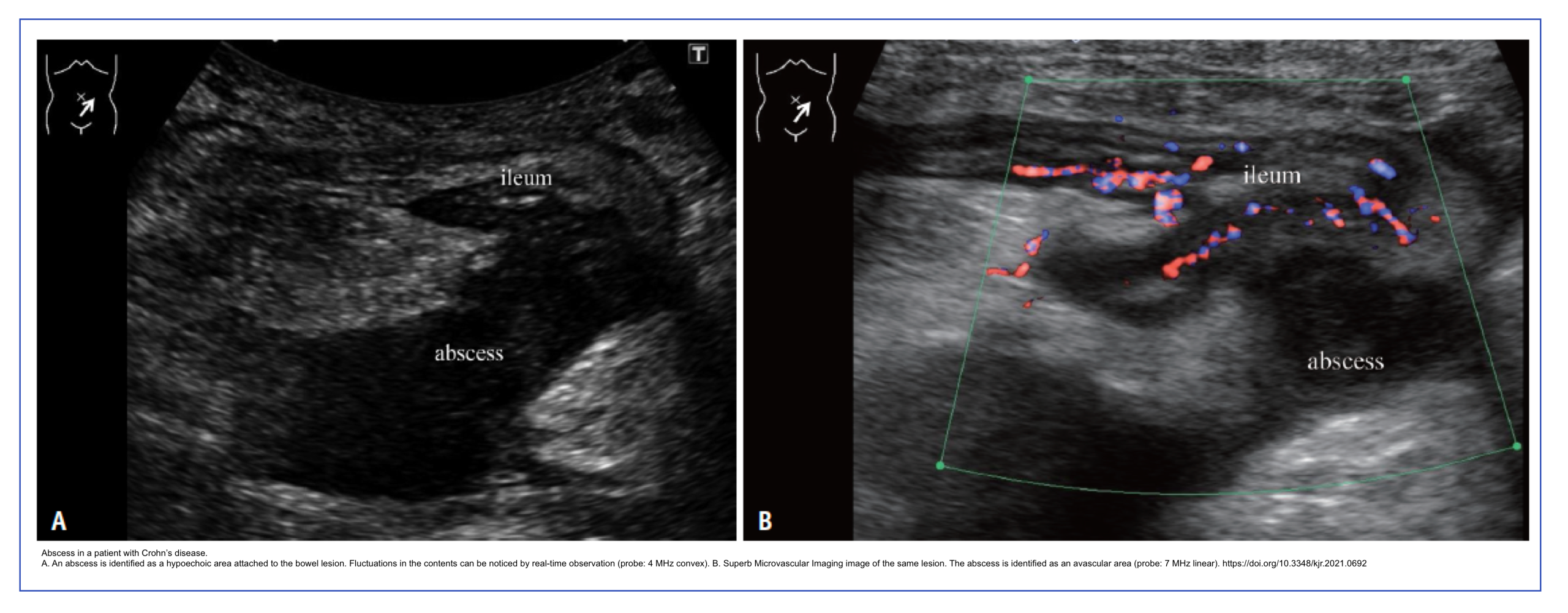
| Abscess | Complex hypoechoic or anechoic collection, may contain internal echoes or air | Complicated diverticulitis, Crohn’s disease, perforated appendicitis |
| Phlegmon | Poorly defined hypoechoic mass, no fluid content, may show vascularity | Severe transmural inflammation without liquefaction |
| Free peritoneal fluid | Anechoic or complex fluid between loops or in dependent spaces | Bowel obstruction, perforation, active inflammation, ischemia |
| Fistula | Hypoechoic tract extending from bowel to adjacent structure (bladder, skin, another loop) | Crohn’s disease, diverticulitis |
| Free air (pneumoperitoneum) | Hyperechoic line with reverberation artifact, enhanced peritoneal stripe | Bowel perforation |

- 💡Clinical significance:
- Inflamed hyperechoic fat is a useful clue, drawing attention to the underlying thickened bowel
- Creeping fat is a highly specific feature of Crohn’s disease
- Presence of an abscess or phlegmon indicates a complicated disease requiring intervention
- CEUS helps differentiate between phlegmon (enhancing) and abscess (avascular)
- Free fluid in obstruction suggests increased risk of strangulation and surgery
Summary table- Intestinal Ultrasound
🔬 Intestinal Ultrasound (IUS) Technique click to expand
📋 1. Overview & Patient Preparation
Intestinal ultrasound (IUS) is a non-invasive, point-of-care tool for assessing transmural inflammation in IBD. It complements endoscopy by visualising the entire bowel wall and detecting complications 1,2.
| Preparation Step | Rationale |
|---|---|
| Fasting (4–8 h) 3 | Reduces gas and food content, improves wall visualisation |
| No fasting (acute abdomen) | Not mandatory in urgent settings |
| Full bladder (optional) | Provides acoustic window for rectum and deep pelvis 4 |
🛠️ 2. Equipment & Optimisation
| Parameter | Setting / Choice | Ref. |
|---|---|---|
| Probe | Curvilinear (1–5 MHz) for overview; Linear (7–12 MHz) for detailed wall layers |
4,5 |
| B‑mode preset | Depth ≤8 cm; focus below target; harmonic imaging ON | 4 |
| Doppler | Low velocity scale (2–5 cm/s); low wall filter; Power Doppler preferred | 4,6 |
🔄 3. Step-by-Step Scanning Technique
Core principle: systematic sweep + graded compression (apply slow, firm pressure to displace gas and assess pliability) 4.
- 1. Overview: Scan solid organs (liver, spleen, kidneys) for incidental findings.
-
2. Colon sweep: Start at the cecum in the right lower quadrant (RLQ).
📍 Landmarks for Cecum: Place the probe just medial to the right Anterior Superior Iliac Spine (ASIS). Look for the iliopsoas muscle (a hypoechoic, strap-like structure) and the iliac artery (pulsatile, anechoic tube) deep to the bowel. The cecum is the blind-ending loop of colon that sits superficial to these structures, often containing gas/feces. -
Trace the colon systematically: ascending → transverse → descending → sigmoid (left lower quadrant).
📍 Landmarks for Sigmoid: In the left lower quadrant, place the probe just medial to the left ASIS. Identify the left iliopsoas muscle and left iliac artery. The sigmoid colon is the curved, S-shaped segment of colon that lies superficial to these structures, often with a thicker wall (up to 4 mm) and visible haustra. - 3. Small bowel: Identify terminal ileum (connects to cecum) → trace proximally using parallel transverse sweeps.
- 4. Graded compression: Apply gentle, steady pressure to evaluate compressibility (normal = pliable; inflamed = rigid) 4.
📊 4. Key Parameters for Inflammation & Vascularity
| Parameter | Normal | Abnormal (Active Disease) |
|---|---|---|
| Bowel Wall Thickness (BWT) | ≤ 3 mm (small bowel & colon) ≤ 4 mm (sigmoid, rectum) |
> 3 mm (small bowel/colon) > 4 mm (sigmoid/rectum) 4,6 |
| Wall Stratification | 5 distinct layers visible (with high‑frequency linear probe) | Loss or disruption of layered pattern 4 |
| Color Doppler Signal (CDS) | Absent or minimal (Limberg 0) | Hyperemia (Limberg 1–3) 6,7 |
| Mesenteric Fat | Not prominent | Hyperechoic, thickened “creeping fat” (specific for CD) 4 |
💎 5. Pearls & Pitfalls
- Be systematic – start at cecum (using ASIS, psoas, iliac artery), follow the colon, then terminal ileum 4.
- Graded compression is your most powerful maneuver.
- Measure BWT perpendicular to the wall – avoid tangential overestimation 4.
- Assess peristalsis in real time – helps differentiate inflammatory vs fibrotic strictures 4.
- Obesity and bowel gas – reduce acoustic window 2,4.
- Operator dependence – requires dedicated training 2.
- Deep segments – rectum, proximal jejunum, and deep pelvis are challenging 4.
- Mimics – thickened wall can be seen in malignancy, ischemia, infection (diverticulitis, appendicitis) 4.
- No dysplasia surveillance – IUS cannot detect mucosal dysplasia 2.
🔧 6. Troubleshooting
| Problem | Solution |
|---|---|
| Excessive gas | Apply graded compression; change patient position (decubitus) 4 |
| Poor depth penetration | Switch to curvilinear probe (1–5 MHz) for deeper loops 4 |
| Motion / breathing artifact | Ask patient to hold breath during Doppler acquisition 4 |
| Difficulty finding a segment | Start from a fixed landmark (ASIS, psoas, iliac vessels) and trace systematically 4 |
📌 7. Quick Reference – Normal vs. Active
| Feature | Normal | Active Inflammation |
|---|---|---|
| BWT | ≤ 3 mm | > 3 mm |
| Stratification | 5 layers preserved | Loss of layers |
| Doppler | Absent (Limberg 0) | Hyperemia (Limberg 1–3) |
| Compressibility | Pliable | Rigid / non-compressible |
| Peristalsis | Present | Reduced or absent |
📚 References & Guidelines
- Maaser C, et al. ECCO-ESGAR Guideline for Diagnostic Assessment in IBD. J Crohns Colitis. 2019;13(2):144-164.
- Lichtenstein GR, et al. ACG Clinical Guideline: Management of Crohn’s Disease in Adults. Am J Gastroenterol. 2025;120(6):1225-1264.
- Rubin DT, et al. ACG Clinical Guideline: Ulcerative Colitis in Adults. Am J Gastroenterol. 2025;120(6):1187-1224.
- Nylund K, et al. EFSUMB Recommendations and Guidelines for Gastrointestinal Ultrasound – Part 1. Ultraschall Med. 2017;38(3):e1-e15.
- AIUM Practice Parameter for the Performance of an Ultrasound Examination of the Abdomen and/or Retroperitoneum. 2022.
- Kucharzik T, et al. Use of Intestinal Ultrasound to Monitor Crohn’s Disease Activity. Clin Gastroenterol Hepatol. 2017;15(4):535-542.
- Calabrese E, et al. Ultrasonography Tight Control and Monitoring in Crohn’s Disease. Clin Gastroenterol Hepatol. 2022;20(3):e711-e722.
Note: All superscript numbers in the text correspond to these references.
Inflammatory Bowel Disease Ultrasound
Overview of IBD and The Role of IUS
Inflammatory bowel disease (IBD) comprises two major disorders: ulcerative colitis (UC) and Crohn disease (CD). UC is traditionally characterized by inflammation limited to the mucosal layer of the colon, while CD is defined by transmural inflammation that can affect any part of the gastrointestinal tract. Both are relapsing and remitting diseases, meaning patients can experience symptomatic remission followed by flares. Over time, chronic inflammation can lead to serious complications—including strictures, fistulas, abscesses, and an increased risk of colorectal cancer—and can significantly impact growth, nutrition, and quality of life, with a variable but often chronic disease course.
However, this classic distinction is now understood to be more nuanced. Evidence from intestinal ultrasound (IUS) and other imaging modalities shows that UC frequently involves the deeper bowel wall, with features such as submucosal thickening, loss of stratification, and mesenteric fibrofatty proliferation. This challenges the “mucosal dogma” and highlights that UC has significant, clinically relevant transmural features *.
This is where Intestinal Ultrasound (IUS) becomes an indispensable tool. Its ability to assess the entire bowel wall thickness, detect loss of stratification, and identify complications like strictures and abscesses makes it uniquely suited to evaluate the transmural nature of both CD and UC. IUS provides a non-invasive, point-of-care window into disease activity that complements endoscopy, which only visualizes the mucosa. By revealing the full thickness of the bowel wall, IUS offers a more complete picture of disease burden, guiding treatment decisions and monitoring response in a way that aligns with the modern, treat-to-target goals of IBD management.
Clinical Case Scenario
Click to expand/collapse case example
Symptoms: Mild intermittent abdominal pain, 2–3 semi-formed stools per day, no bleeding, no urgency, no weight loss
Last colonoscopy (18 months prior): Mild terminal ileitis (SES-CD 4)
Current therapy: Adalimumab 40 mg every 2 weeks
❌ Without IUS (Standard Care Pathway)
| Time Point | Event | Consequence |
|---|---|---|
| Baseline | Patient reports mild symptoms only | Clinician assumes clinical remission |
| Month 0 | CRP and fecal calprotectin ordered | Results delayed by 2 weeks |
| Month 0.5 | CRP normal, FC moderately elevated (250 µg/g) | Uncertainty: false positive? subclinical inflammation? |
| Month 1 | Colonoscopy scheduled | Wait time 6 weeks |
| Month 2.5 | Colonoscopy: severe terminal ileum stricture (SES-CD 12) with prestenotic dilation | Diagnosis of fibrostenotic complication |
| Month 3 | MR enterography ordered to assess stricture extent | Additional 3-week wait |
| Month 4 | MRE confirms 8 cm fibrotic stricture with upstream dilation | Patient now has intermittent obstructive symptoms |
| Month 4.5 | Ileocecal resection | Prolonged hospitalization, 8 weeks missed work |
✅ With IUS (Point-of-Care Pathway)
| Time Point | Event | Benefit / Outcome |
|---|---|---|
| Baseline | Patient reports mild symptoms | – |
| Same day | IUS performed in clinic | Immediate result |
| Same day | IUS findings: BWT 7 mm, Limberg score 1, luminal narrowing 8 mm with prestenotic dilation (3.5 cm) | Diagnosis: fibrotic stricture (not active inflammation) |
| Same day | Clinical decision made: stop adalimumab, refer to surgery | Avoids unnecessary biologic escalation |
| Same day | No need for MRE or repeat colonoscopy | Saves cost, time, and patient burden |
| Week 2 | Elective laparoscopic strictureplasty | Planned surgery, shorter hospitalization, faster recovery (3 weeks to work) |
• Symptoms alone are unreliable – Mild symptoms masked a severe fibrotic stricture
• Biomarkers can mislead – Normal CRP, mildly elevated FC created diagnostic uncertainty
• IUS accelerates care – 4.5 months to surgery without IUS vs. 2 weeks with IUS
• IUS prevents unnecessary escalation – Adalimumab (ineffective for fibrosis) was stopped
• IUS reduces testing burden – No need for colonoscopy or MRE when IUS is diagnostic
• Better patient outcome – Elective surgery, fewer complications, faster recovery
“Clinical symptoms and biomarkers alone are insufficient to guide therapy in Crohn’s disease. This patient’s mild symptoms masked a severe fibrotic stricture that required surgery. Point-of-care IUS provided immediate diagnosis, prevented unnecessary biologic escalation, expedited surgical referral, and improved the patient’s outcome. Delaying objective assessment leads to disease progression, complications, and avoidable morbidity.”
1. Lichtenstein GR, et al. ACG clinical guideline: management of Crohn’s disease in adults. Am J Gastroenterol. 2025;120(6):1225-1264.
2. Turner D, et al. STRIDE-II: an update on the selecting therapeutic targets in IBD. Gastroenterology. 2021;160(5):1570-1583.
3. Friedman AB, et al. Effect of point-of-care gastrointestinal ultrasound on decision-making and management in inflammatory bowel disease. Aliment Pharmacol Ther. 2021;54(5):652-666.
4. Novak KL, et al. Clinic-based point of care transabdominal ultrasound for monitoring Crohn’s disease: impact on clinical decision making. J Crohns Colitis. 2015;9(9):795-801.
Rationale For Using IUS in IBD
◾️Why ultrasound in IBD?
- IBD requires frequent objective monitoring — clinical symptoms alone are unreliable (up to 25% of asymptomatic patients have active inflammation)
- Endoscopy is invasive, costly, and impractical for serial follow-up
- CT exposes young patients to cumulative radiation
- IUS is non-invasive, radiation-free, low-cost, repeatable, and patient-preferred
⎮ECCO-ESGAR (2025) and ACG (2025) recognize IUS as a first-line tool for assessing disease activity and complications in IBD.
◾️What IUS can do in IBD
- IUS in Crohn’s disease *
- Detect and localize small bowel and colonic inflammation
- Assess disease extent (sensitivity 86–94%, specificity 94–97%)
- Identify complications: strictures, fistulas, abscesses (comparable to MRE/CT)
- Monitor response to biologic therapy as early as 4–12 weeks
- Detect postoperative recurrence (BWT >3–5.5 mm predicts Rutgeerts ≥ i2b *)
- IUS in ulcerative colitis *
- Evaluate disease extension (especially when colonoscopy is incomplete)
- Monitor treatment response — changes seen as early as 2 weeks
- Assess for colonic wall thickening (BWT >3 mm) and hyperemia
- Milan Ultrasound Criteria (MUC >6.2) predict endoscopic activity with 100% specificity *
- Milan Ultrasound Criteria (MUC) is a quantitative score calculated from IUS parameters (BWT and bowel wall flow, “BWF”) using the formula: MUC = 1.4 × BWT + 2 × BWF.
- A MUC >6.2 predicts endoscopic activity with 100% specificity. MUC >6.2 at baseline also predicts a 3.87-fold higher risk of adverse outcomes (treatment escalation, corticosteroids, hospitalization, or colectomy).
- Milan Ultrasound Criteria (MUC) is a quantitative score calculated from IUS parameters (BWT and bowel wall flow, “BWF”) using the formula: MUC = 1.4 × BWT + 2 × BWF.
- Transperineal US evaluates rectal inflammation (BWT ≥4 mm) *
- More on IUS in UC, see here
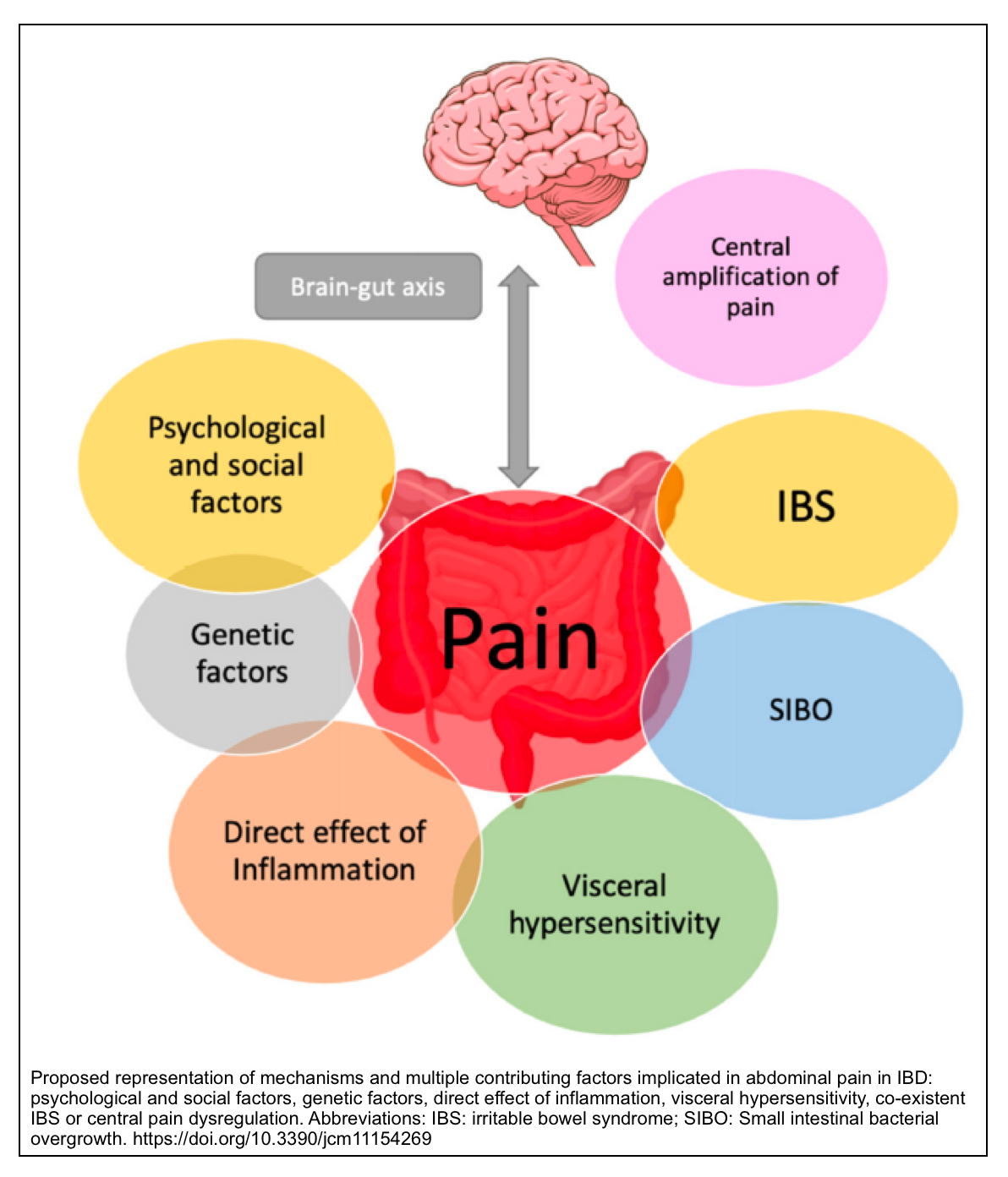
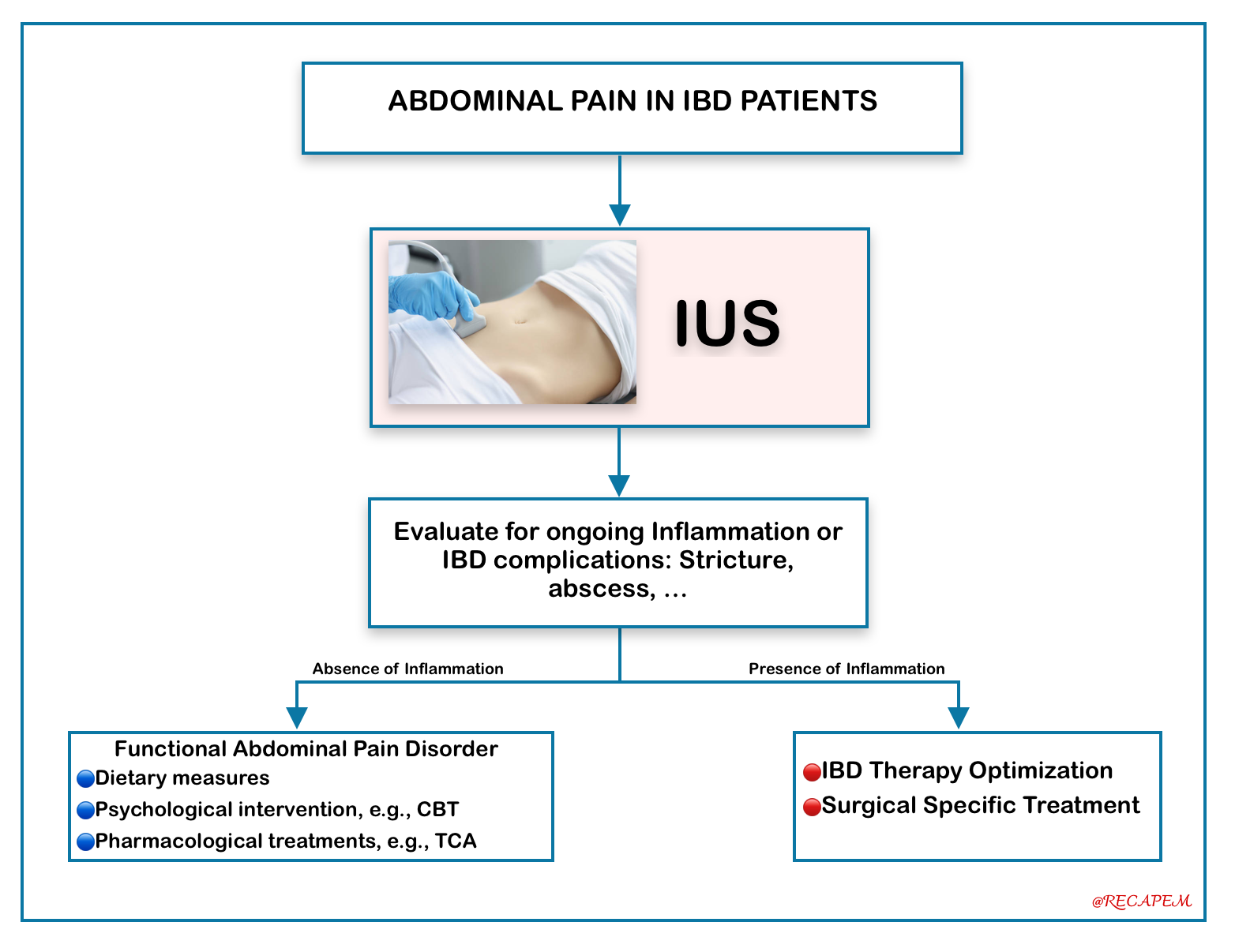
- Differentiating Active Inflammation from Functional Symptoms
- While the hallmark symptoms of IBD (abdominal pain, diarrhea, rectal bleeding, and urgency) drive treatment during flares, a significant proportion of patients in remission continue to experience these issues due to functional gastrointestinal symptoms or IBS-type symptoms. Pathophysiology of functional symptoms is shown in the figure below.
- A normal IUS—defined by a BWT ≤3 mm and an absent Doppler signal—has a very high negative predictive value and effectively rules out active transmural inflammation, providing a crucial distinction between a true flare and a functional disorder *.
- While the hallmark symptoms of IBD (abdominal pain, diarrhea, rectal bleeding, and urgency) drive treatment during flares, a significant proportion of patients in remission continue to experience these issues due to functional gastrointestinal symptoms or IBS-type symptoms. Pathophysiology of functional symptoms is shown in the figure below.
📍Pathophysiology of Functional Symptoms in IBD and IUS Clinical Implications in IBD Patients with Abdominal Pain
⚠️Limitations of IUS in IBD
- Limited visualization of the rectum, proximal jejunum, and deep pelvis
- Operator-dependent (requires dedicated training)
- Less accurate for disease length measurement in extensive small bowel CD
- Not suitable for dysplasia surveillance
- Obesity may limit image quality
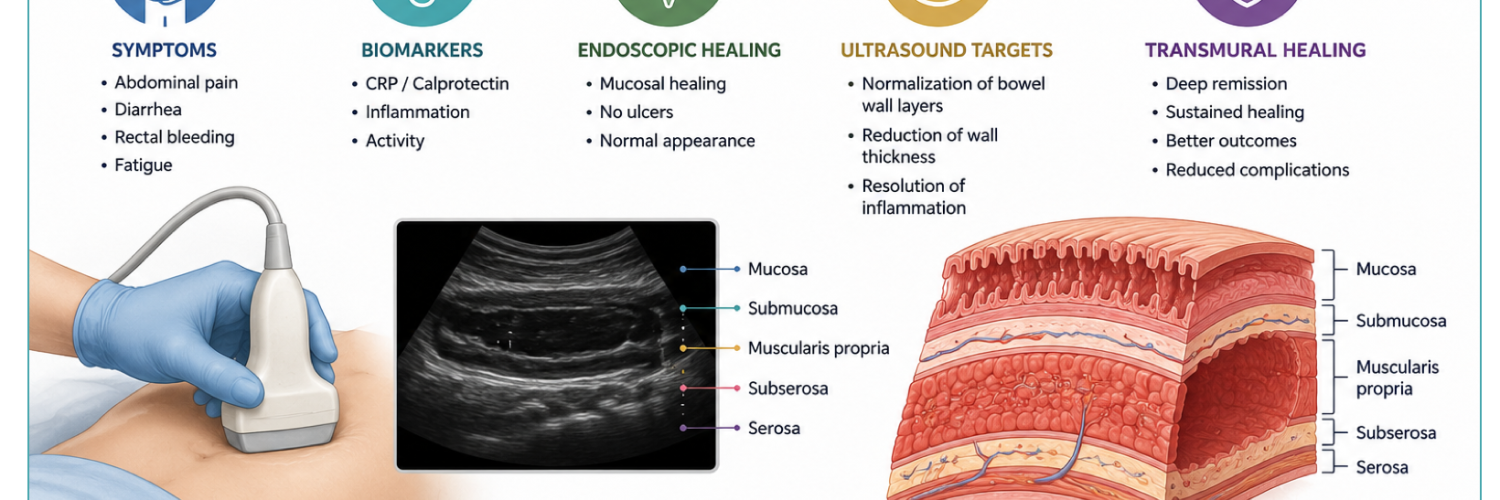
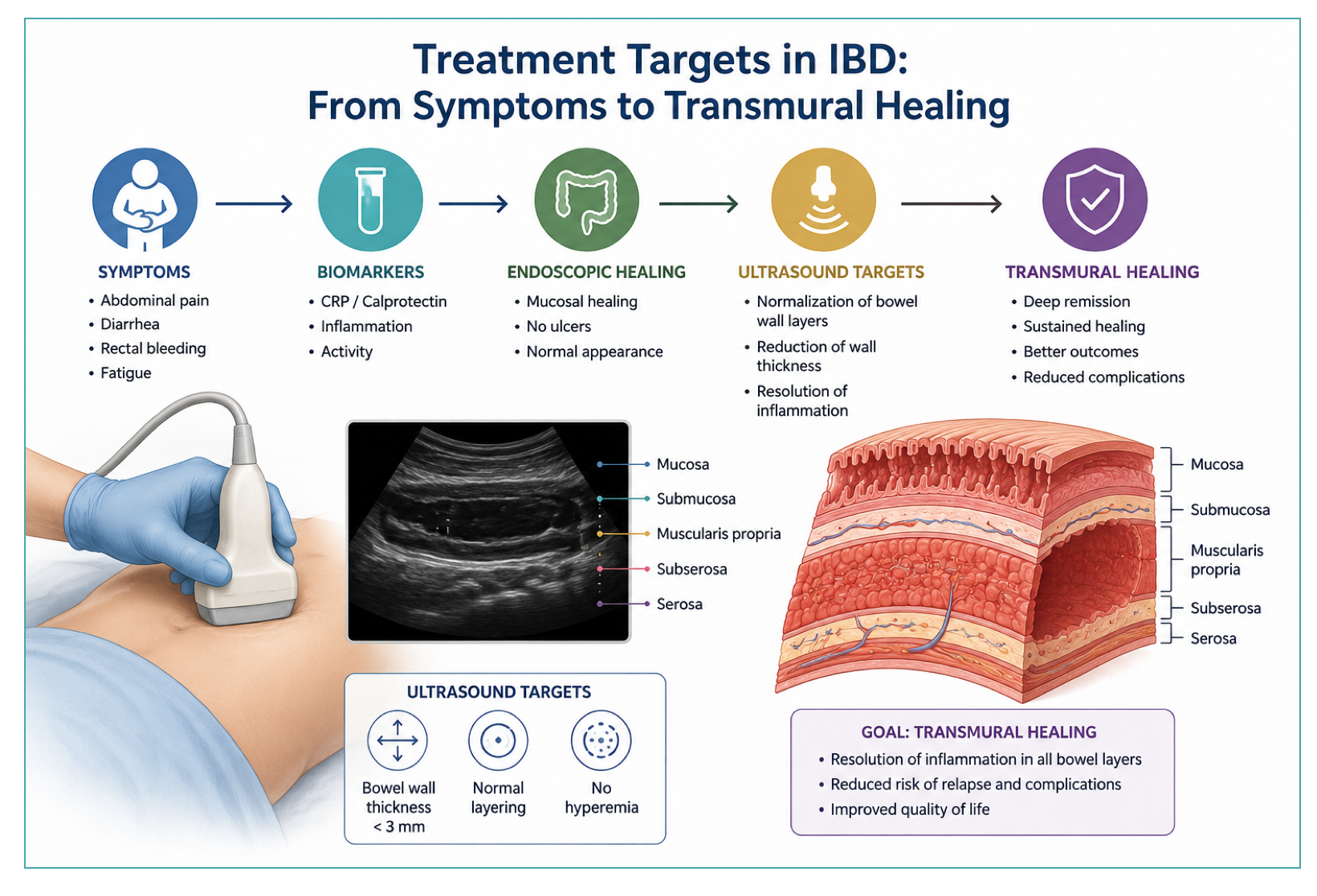
Treatment Targets in IBD
🎯Treatment Target Strategy in IBD: Deep Remission
- Deep Remission: This is the combination of clinical remission + endoscopic healing while being corticosteroid-free. Studies show this significantly reduces disease progression.
- According to the latest STRIDE-II consensus and major society guidelines, the “gold standard” test for IBD remission is Endoscopic Healing (also known as Mucosal Healing).
- This is the primary long-term target because it directly correlates with improved clinical outcomes, reduced hospitalization rates, and a lower risk of surgery.
- According to the latest STRIDE-II consensus and major society guidelines, the “gold standard” test for IBD remission is Endoscopic Healing (also known as Mucosal Healing).
- Emerging Targets
- Transmural Healing (CD): Because Crohn’s affects the full thickness of the bowel wall, there is growing evidence that achieving Transmural Healing (normalization of the bowel wall on Ultrasound or MRI/MRE) leads to even better long-term outcomes than mucosal healing alone. However, it is currently considered an adjunctive target rather than a mandatory gold standard *.
- Endoscopy sees only the mucosa (inner lining).
- MRE sees the entire bowel wall (mucosa + submucosa + muscularis + serosa) and surrounding mesentery.
- MRE is the gold standard imaging test to confirm Transmural Healing.
- Is MRE recommended for routine monitoring? Not for all patients. It is reserved for specific scenarios (see below).
- Histologic Healing (UC): While STRIDE-II does not mandate it as a formal target, histological remission (normalization of tissue under the microscope) is emerging as a deeper goal for Ulcerative Colitis to predict even lower relapse rates
- Transmural Healing (CD): Because Crohn’s affects the full thickness of the bowel wall, there is growing evidence that achieving Transmural Healing (normalization of the bowel wall on Ultrasound or MRI/MRE) leads to even better long-term outcomes than mucosal healing alone. However, it is currently considered an adjunctive target rather than a mandatory gold standard *.
📍NOTE: Clinical Significance of Transmural Healing as a Therapeutic Target
Click to expand/collapse table
| Finding | Evidence |
|---|---|
| CD is a transmural disease | Inflammation extends beyond mucosa to muscularis and serosa |
| Mucosal healing does not equal transmural healing | Up to 25% of patients with endoscopic remission have persistent transmural inflammation on IUS |
| Transmural healing predicts better outcomes | Lower rates of surgery, hospitalization, and corticosteroid use (Castiglione 2019, Zorzi 2020) |
| Persistent transmural inflammation increases risk of complications | Strictures, fistulas, abscesses |
Click to expand/collapse table
| Indication | Rationale | Alternative Modality |
|---|---|---|
| Known or suspected small bowel Crohn’s disease | Colonoscopy cannot reach proximal small bowel (jejunum, proximal ileum) | CT enterography, Capsule endoscopy, IUS (limited for proximal) |
| Suspected penetrating complications (fistula, abscess, phlegmon) | MRE has high sensitivity for detecting fistulous tracts and fluid collections | CT, IUS with CEUS, Pelvic MRI (for perianal) |
| Suspected stricturing disease (fibrotic vs. inflammatory) | MRE can assess degree of fibrosis (dark stricture) vs. inflammation (enhancement, edema) | CT enterography, IUS with elastography (emerging) |
| Incomplete colonoscopy (terminal ileum not intubated) | MRE assesses the ileum and proximal colon when endoscopy cannot reach | CT enterography, Capsule endoscopy (if no stricture) |
| Postoperative CD monitoring (ileocolic resection) | Assess neoterminal ileum and anastomosis for recurrence (Rutgeerts score surrogate) | Colonoscopy (gold standard), IUS |
| Pregnancy (avoiding radiation) | MRE is preferred over CT in pregnant patients when imaging is necessary | IUS (first-line, safe), Limited MRI |
| Extraintestinal manifestations (hepatobiliary, pancreatic) | MRE can assess for PSC, cholelithiasis, pancreatitis, or other complications | Abdominal ultrasound (first-line), CT, MRCP |
| Young patients requiring serial examinations | No ionizing radiation (unlike CT), preferred for patients <35 years | IUS (preferred for frequent monitoring), CT (avoid due to radiation) |
| Assessment of transmural healing (research/adjunctive target) | MRE can document normalization of bowel wall thickness and enhancement | IUS (emerging, point-of-care) |
| Perianal CD (pelvic MRI) | Pelvic MRI is gold standard for classifying perianal fistulas and abscesses | Transperineal ultrasound (TPUS), Endoanal ultrasound (EAUS), CT |
Defining Treat-To-Target Strategy
The Treat-to-Target strategy is the modern, evidence-based framework for managing IBD. Rather than simply treating symptoms, this approach sets specific, measurable goals and escalates therapy until those goals are achieved.
The Four Targets:
- Clinical Remission (Immediate)
- Symptom resolution (e.g., HBI < 5, normal stool frequency).
- ⚠️This is insufficient alone, since up to 25% of asymptomatic patients have active inflammation.
- Symptom resolution (e.g., HBI < 5, normal stool frequency).
- Biochemical Remission (Intermediate)
- Normalization of Fecal Calprotectin (< 100–250 µg/g) and CRP (< 5 mg/L).
- ⚠️Useful for monitoring but cannot localize disease or detect complications.
- Normalization of Fecal Calprotectin (< 100–250 µg/g) and CRP (< 5 mg/L).
- Mucosal Healing (Primary Gold Standard)
- Endoscopic normalization via colonoscopy (SES-CD < 3 or no ulcers for CD; Mayo 0–1 for UC).
- ✅Correlates with reduced hospitalization and surgery.
- Endoscopic normalization via colonoscopy (SES-CD < 3 or no ulcers for CD; Mayo 0–1 for UC).
- Transmural Healing (Adjunctive/Deep)
- Full bowel wall normalization on IUS (BWT ≤ 3 mm + no Doppler signal) or MRE.
- 🚨Associated with even better outcomes but not yet a formal STRIDE-II target.
- Full bowel wall normalization on IUS (BWT ≤ 3 mm + no Doppler signal) or MRE.
⎮In this framework, IUS findings directly inform clinical decisions: active inflammation (e.g., BWT >3 mm with Doppler signal) guides treatment escalation, while sustained transmural remission (BWT ≤3 mm, no Doppler signal) supports the safe consideration of treatment de-escalation.”
Monitoring Modalities and Tools
Achieving IBD remission is no longer defined by a single test. Instead, it is a multi-tiered “Treat-to-Target” strategy that combines several layers of evidence to confirm disease control. Here are the gold standard tests for the key targets in IBD management:
🎯Long-Term Gold Standard: Colonoscopy
- This is the definitive test for remission. It involves direct visual inspection of the intestinal lining. Guidelines define remission by specific scores:
- Crohn’s Disease (CD): SES-CD < 3 or the absence of ulcerations
- Ulcerative Colitis (UC): Mayo Endoscopic Score (MES) of 0 (normal mucosa) or 1 (mild friability/erythema)
🎯Intermediate/Short-Term Targets (Non-Invasive)
- Since colonoscopy is invasive and costly, these tests are used for frequent monitoring to confirm that treatment is working.
- Fecal Calprotectin: This is the most reliable non-invasive biomarker. It measures inflammation directly in the gut.
- Target: Usually < 100–250 µg/g
- Serum CRP: Normalization of C-Reactive Protein levels (typically < 5 mg/L)
- Intestinal Ultrasound (IUS): A radiation-free, point-of-care tool gaining prominence. Remission is defined as Bowel Wall Thickness (BWT) ≤ 3 mm with no Doppler signal (normalization of wall structure)
- Fecal Calprotectin: This is the most reliable non-invasive biomarker. It measures inflammation directly in the gut.
🎯Clinical & Patient-Reported (PRO) Targets Are Immediate Goals
- While not sufficient alone to define remission (due to symptom-inflammation discordance), resolution of symptoms is a mandatory immediate goal.
- CD: Harvey-Bradshaw Index (HBI) < 5 or PRO2 normalization (Abdominal pain ≤ 1, Stool frequency ≤ 3)
- UC: Partial Mayo Score < 3 with no rectal bleeding and normal/near-normal stool frequency
Click to expand/collapse table
| Modality | Target | Formal STRIDE-II Target? | Definition of Remission | Best For / Limitations |
|---|---|---|---|---|
| Colonoscopy | Mucosal healing | ✅ Yes (primary) |
CD: SES-CD <3 or no ulcers UC: Mayo score 0 or 1 |
Best for: All colonic/ileal CD and UC Limitations: Invasive, costly, cannot be repeated frequently, sedation required |
| MRE | Transmural healing | ❌ No (adjunctive) | BWT ≤3 mm, resolution of abnormal enhancement, no edema, no active complications |
Best for: Small bowel CD, fistulas, abscesses, strictures Limitations: Costly, limited access, claustrophobia, not for routine monitoring |
| Intestinal Ultrasound (IUS) | Transmural healing | ❌ No (adjunctive) | BWT ≤3 mm AND absent/grade 0 color Doppler signal |
Best for: Point-of-care, frequent monitoring, pregnancy, pediatrics Limitations: Operator dependent, limited for rectum and proximal jejunum |
| Fecal Calprotectin (FC) | Biochemical remission | ✅ Yes (intermediate) | <100–250 µg/g (correlates with mucosal healing) |
Best for: Non-invasive monitoring, frequent use, treatment response Limitations: Cannot localize disease, false positives (NSAIDs, infections), does not detect complications |
| C-Reactive Protein (CRP) | Biochemical remission | ✅ Yes (intermediate) | Normalization (<5 mg/L or ULN per local assay) |
Best for: Easy, cheap, widely available Limitations: 20–30% false negative in active CD, nonspecific (infections, arthritis) |
| Clinical Symptoms (PRO2, HBI, partial Mayo) | Clinical remission | ✅ Yes (immediate) |
CD: HBI <5 or PRO2 normal (pain ≤1, stools ≤3) UC: PRO2 bleeding 0, stools normal/near normal |
Best for: Immediate assessment, every visit Limitations: Subjective, recall bias, discordant with inflammation in up to 25% of patients |
Endoscopic healing remains the primary formal target. Transmural healing (MRE/IUS) is an adjunctive target, not yet mandatory. Clinical and biochemical targets are intermediate/short-term.
IUS
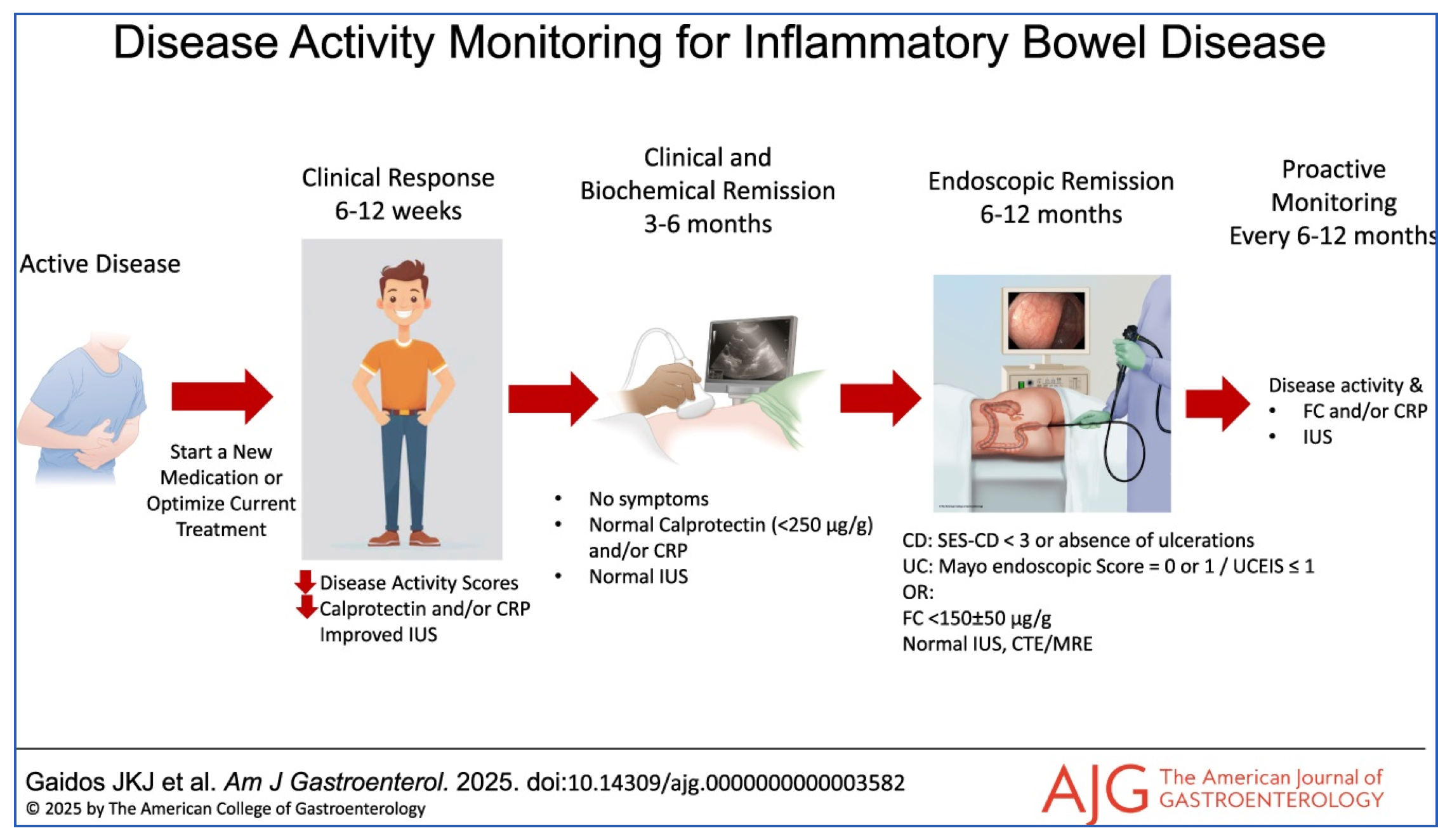
Definitions of response and remission based on IUS evaluation (IUS consensus 2022)
- US response (at 12–14 weeks):
- Reduction in BWT by ≥25% OR ≥2.0 mm OR
- Reduction ≥1.0 mm + decrease in Limberg score by ≥1 grade
- IUS transmural remission (at 26–52 weeks):
- BWT ≤3 mm AND
- Normal/absent color Doppler signal
⎮Transmural healing (TH) is associated with lower rates of surgery, hospitalization, and corticosteroid use
Evidence
Click to expand/collapse table
| Study / Source | Key Finding |
|---|---|
| ECCO-ESGAR 2019 | IUS recommended for initial diagnosis and monitoring of CD |
| ACG 2025 (CD guideline) | IUS is an adjunct for diagnosis and response monitoring (Key Concept #32) |
| ACG 2025 (UC guideline) | IUS can assess disease activity and response (Key Concept #8) |
| TRUST (Kucharzik 2017) | IUS normalized within 3 months in responders; BWT reduction correlated with CRP |
| STARDUST (Kucharzik 2023) | IUS response at week 4 predicted week 48 endoscopic response (NPV 73%) |
| METRIC trial (Taylor 2018) | IUS vs MRE comparable for terminal ileum disease (sensitivity 92% vs 97%) |
| Calabrese 2022 | Transmural healing at 12 months associated with lower surgery and hospitalization |
| Maaser 2020 (TRUST&UC) | BWT improvement seen at 2 weeks post-treatment in UC |
| de Voogd 2022 | BWT <2.8 mm predicted endoscopic remission in UC (AUC 0.87) |
| Rispo 2018 (meta-analysis) | IUS for postoperative CD recurrence: sensitivity 94%, specificity 84% |
| Maconi 2017 (meta-analysis) | TPUS for perianal fistulas: sensitivity 98.3%, specificity 92.8% |
Full References:
1. Maaser C, et al. ECCO-ESGAR Guideline for Diagnostic Assessment in IBD Part 1: Initial diagnosis, monitoring of known IBD, detection of complications. J Crohns Colitis. 2019;13(2):144-164.
2. Lichtenstein GR, et al. ACG clinical guideline: management of Crohn’s disease in adults. Am J Gastroenterol. 2025;120(6):1225-1264.
3. Rubin DT, et al. ACG clinical guideline: ulcerative colitis in adults. Am J Gastroenterol. 2025;120(6):1187-1224.
4. Kucharzik T, et al. Use of intestinal ultrasound to monitor Crohn’s disease activity. Clin Gastroenterol Hepatol. 2017;15(4):535-542.e2.
5. Kucharzik T, et al. Early ultrasound response and progressive transmural remission after treatment with ustekinumab in Crohn’s disease. Clin Gastroenterol Hepatol. 2023;21(1):153-163.e12.
6. Taylor SA, et al. Diagnostic accuracy of magnetic resonance enterography and small bowel ultrasound for the extent and activity of newly diagnosed and relapsed Crohn’s disease (METRIC): a multicentre trial. Lancet Gastroenterol Hepatol. 2018;3(8):548-558.
7. Calabrese E, et al. Ultrasonography tight control and monitoring in Crohn’s disease during different biological therapies: a multicenter study. Clin Gastroenterol Hepatol. 2022;20(3):e711-e722.
8. Maaser C, et al. Intestinal ultrasound for monitoring therapeutic response in patients with ulcerative colitis: results from the TRUST&UC study. Gut. 2020;69(9):1629-1636.
9. de Voogd F, et al. Intestinal ultrasound is accurate to determine endoscopic response and remission in patients with moderate to severe ulcerative colitis: a longitudinal prospective cohort study. Gastroenterology. 2022;163(6):1569-1581.
10. Rispo A, et al. Diagnostic accuracy of ultrasonography in the detection of postsurgical recurrence in Crohn’s disease: a systematic review with meta-analysis. Inflamm Bowel Dis. 2018;24(5):977-988.
11. Maconi G, et al. Transperineal ultrasound for perianal fistulas and abscesses – a systematic review and meta-analysis. Ultraschall Med. 2017;38(3):265-272.
IUS vs. Biochemical Markers (CRP and Fecal Calprotectin)
- Why Biomarkers Alone Are Insufficient
- CRP: Normal in 20–30% of patients with endoscopically active CD; nonspecific (elevated in infections, arthritis, etc.)
- Fecal calprotectin (FC): More sensitive than CRP, but cannot localize disease, cannot detect complications (strictures, fistulas, abscesses), and levels vary by disease extent and location
- When biomarkers are used for monitoring IBD activity, still 50% of patients don’t meet the primary outcome (i.e., deep remission: CDEIS <4 and no deep ulcers at 48 weeks) *.
Click to expand/collapse table
| Parameter | CRP | Fecal Calprotectin | IUS |
|---|---|---|---|
| Real-time result | No (hours–days) | No (hours–days) | Yes (immediate) |
| Localizes disease | No | No | Yes (anatomical segments) |
| Detects complications | No | No | Yes |
| Transmural assessment | No | No | Yes |
| Correlation with endoscopy | Moderate (30% false negative) | Good (r = 0.60–0.75) | High (r = 0.70–0.85) |
| Operator dependent | No | No | Yes |
| Cost | Low | Moderate | Low |
IUS vs. Clinical signs & symptoms
Click to expand/collapse table
| Parameter | Clinical Symptoms/Signs | IUS |
|---|---|---|
| Real-time result | Yes | Yes |
| Objective | No (subjective, recall bias) | Yes (measurable BWT, Doppler) |
| Detects subclinical inflammation | No | Yes |
| Localizes disease | Poor (vague abdominal pain) | Yes (anatomical segments) |
| Assesses severity | Limited (stool frequency, pain scales) | Yes (BWT in mm, Limberg grade) |
| Detects complications (strictures, fistulas, abscesses) | No (often silent) | Yes |
| Differentiates inflammation from functional symptoms | No | Yes |
| Patient burden | None (history only) | Minimal (no prep, no sedation, no radiation) |
IUS vs. MRE
Click to expand/collapse table
| Parameter | IUS | MRE / MRI |
|---|---|---|
| Radiation exposure | ✅ None | ✅ None |
| Contrast agent required | No (optional for CEUS) | Yes (IV gadolinium ± oral contrast) |
| Patient preparation | None (fasting optional) | Fasting + oral contrast ingestion (45–60 min before) |
| Examination time | 5–20 minutes | 30–60 minutes |
| Real-time imaging | ✅ Yes (dynamic assessment of peristalsis, compressibility) | ❌ No (static images, cine clips limited) |
| Point-of-care availability | ✅ Yes (can be performed in clinic by gastroenterologist) | ❌ No (requires radiology department appointment) |
| Cost | Low | High |
| Sensitivity for terminal ileum CD | 92% (METRIC trial) | 97% (METRIC trial) |
| Sensitivity for colonic CD | 67–74% (superior to MRE for colon) | 47–53% (limited for colonic assessment) |
| Detection of small bowel disease extent | 70% (limited for proximal jejunum) | 80% (superior for proximal small bowel) |
| Detection of strictures | Comparable to MRE (kappa = 0.82) | Comparable to IUS (kappa = 0.82) |
| Detection of fistulas | Comparable (kappa = 0.67) | Comparable, slightly superior for deep pelvic fistulas |
| Detection of abscesses | Comparable (kappa = 0.88) | Comparable, superior for deep pelvic abscesses |
| Perianal CD assessment | TPUS: sensitivity 98%, specificity 93% (alternative) | Pelvic MRI: gold standard for fistula classification |
| Interobserver agreement | Good (kappa = 0.64 for CD, 0.87 for UC) | Modest (kappa = 0.36–0.56 for CD) |
| Repeatability for frequent monitoring | Excellent (can be repeated weekly/monthly) | Limited (cost, access, patient burden) |
| Patient preference / tolerability | Highly preferred (no claustrophobia, no contrast, no fasting) | Less preferred (claustrophobia, loud noise, long duration) |
| Limitations | Operator dependent, limited for rectum/proximal jejunum, obesity | Limited access, contraindications (pacemaker, claustrophobia), less accurate for colon |
IUS vs. endo/colonoscopy
Click to expand/collapse table
| Parameter | IUS | Endoscopy / Colonoscopy |
|---|---|---|
| Invasiveness | ✅ Non-invasive (transabdominal) | ❌ Invasive (requires intubation, sedation) |
| Patient preparation | None (fasting optional) | Full bowel preparation + fasting + sedation/anesthesia |
| Risk of complications | None | Perforation (0.1–0.3%), bleeding, sedation-related risks, infection |
| What is assessed | Transmural (full bowel wall: mucosa, submucosa, muscularis, serosa, mesentery) | Mucosal surface only (cannot assess deeper layers) |
| Assessment of small bowel beyond TI | ✅ Yes (sweeping technique, limited for proximal jejunum) | ❌ No (standard colonoscopy only reaches terminal ileum) |
| Detection of complications | Strictures, fistulas, abscesses, creeping fat (comparable to MRE/CT) | Limited (cannot assess extraluminal complications well) |
| Assessment of peristalsis / motility | ✅ Yes (real-time dynamic assessment) | ❌ No (static examination) |
| Graded compression (pliability) | ✅ Yes (assesses compressibility, rigid vs. pliable) | ❌ No |
| Tissue sampling (biopsy) | ❌ No | ✅ Yes (histology, dysplasia surveillance, CMV testing) |
| Therapeutic intervention | ❌ No (diagnostic only) | ✅ Yes (dilation, polypectomy, hemostasis, stricturotomy) |
| Correlation with inflammation | High (r = 0.70–0.85 with endoscopy) | Gold standard reference |
| Scoring system for disease activity |
⚠️ No universally validated total score Available: Limberg score (vascularity only), SUS-CD, MUC, IBUS-SAS (research) None equivalent to SES-CD or Mayo score |
✅ Validated scores exist CD: SES-CD (0–60), CDEIS UC: Mayo score (0–3), UCEIS (0–8) |
| STRIDE-II formal target | ❌ No (adjunctive target for transmural healing) | ✅ Yes (primary target for mucosal healing) |
| Sensitivity for detecting active CD | 85–94% (depending on location) | 95–100% (reference standard, but limited to mucosa) |
| Specificity for detecting active CD | 91–97% | 95–100% (with histology) |
| Repeatability for frequent monitoring | ✅ Excellent (can be repeated weekly/monthly) | ❌ Limited (invasive, costly, patient burden, risks) |
| Cost | Low (∼$60–150) | High (∼$350–850 + sedation, facility fees) |
| Patient preference | Highly preferred (no preparation, no sedation, no pain) | Less preferred (preparation, sedation, discomfort) |
| Limitations | Operator dependent, limited for rectum/proximal jejunum, obesity, no biopsy, no validated total score | Invasive, requires sedation, cannot assess transmural healing, cannot assess proximal small bowel, risk of complications |
📍Note: No Total IUS Score Equivalent to Total SES-CD
- There is no IUS score equivalent of the total SES-CD score for the entire visualized bowel, and limits correlation between the two measures
- Segmental BWT on IUS is accurate in detecting endoscopic inflammation based on the segmental SES-CD score
- Several segmental IUS activity scores have been recently developed, but lack sufficient external validation with the segmental SES-CD
- 🔗 IBD SCORES
IUS Parameters
- The full list of indices is listed in the following table.
- However, in practice, despite different scoring systems, 2 indices are used for IBD activity monitoring: BWT and bowel wall hyperemia (this is graded by the modified Limberg score).
Click to expand/collapse table
| Parameter | Normal | Active Disease |
|---|---|---|
| Bowel wall thickness (BWT) | ≤3 mm (ileum/colon) ≤4 mm (rectum) |
>3 mm (ileum/colon) >4 mm (rectum) |
| Hyperemia (Limberg score) | 0 (absent) | 1–3 (present) |
| Bowel wall stratification | Preserved (5 layers) | Focal or complete loss |
| Mesenteric fat (creeping fat) | Absent | Hyperechoic, surrounding bowel |
| Lymph nodes | Short axis <4 mm | Enlarged, oval, hypoechoic |
Ultrasound Scoring Systems in IBD
- To standardize disease activity assessment and treatment response, several semi-quantitative and quantitative scoring systems have been developed.
- Modified Limberg Score (Doppler Grading)
- The most widely used semi-quantitative grading system for bowel wall vascularity 👇:
Click to expand/collapse table
| Grade | Description | Interpretation |
|---|---|---|
| 0 | No bowel wall thickening, no color Doppler signal | Normal |
| 1 | Bowel wall thickening (>3 mm), but no detectable color Doppler signal | Inactive or quiescent |
| 2 | Bowel wall thickening + short stretches / small spots of color Doppler signal within the wall | Mild-to-moderate active inflammation |
| 3 | Bowel wall thickening + long stretches of color Doppler signal within the wall | Severe active inflammation |
| 4 | Bowel wall thickening + long stretches of color Doppler signal extending into the mesentery | Severe active inflammation with mesenteric involvement |
IUS in Special Population
Click to expand/collapse table
| Population | Utility / Key Points |
|---|---|
| Pregnancy | Safe; good visualization of colon (91%) and terminal ileum in first 2 trimesters |
| Pediatrics | No sedation; normal BWT ≤2–2.5 mm; correlates with endoscopic activity |
| Postoperative CD | BWT ≥3 mm suggests recurrence; ≥5–6 mm suggests severe recurrence (Rutgeerts i3–i4) |
| Perianal CD | TPUS accurate for abscesses and fistulas (sensitivity 98%, specificity 93%); alternative to MRI when unavailable |
Practical Approach
Multimodal Monitoring for IBD activity
Multimodal monitoring is the cornerstone of modern IBD management. It recognizes that no single test is sufficient to accurately assess disease activity or guide treatment decisions. Instead, it integrates multiple, complementary layers of information:
- Clinical assessment (symptoms, patient-reported outcomes)
- Biochemical markers (Fecal Calprotectin, CRP)
- Endoscopic evaluation (mucosal healing on colonoscopy)
- Transmural imaging (Intestinal Ultrasound, MRE)
Why is this integration crucial?
- Relying on any single modality can be misleading.
- Symptoms are subjective and may not reflect active inflammation (up to 25% of asymptomatic patients have active disease).
- Biomarkers are useful but cannot localize inflammation or detect complications like strictures or fistulas.
- Endoscopy is the gold standard for the mucosa but is invasive and cannot assess the deeper bowel wall.
- IUS provides a unique, real-time, non-invasive view of transmural healing and complications.
By combining these tools, the clinician can:
- Rule out active inflammation in a symptomatic patient (identifying functional symptoms).
- Detect subclinical inflammation in an asymptomatic patient, allowing early intervention.
- Differentiate inflammatory from fibrotic strictures, guiding appropriate therapy (medical vs. surgical).
- Confirm true remission when all modalities are normal, allowing for confident treatment de-escalation.
The table below provides a practical, scenario-based guide to interpreting the combination of clinical presentation, CRP, Fecal Calprotectin, and IUS findings, and outlines the recommended clinical action for each situation.
Click to expand/collapse table
| Clinical Presentation | CRP | FC | IUS Finding | Interpretation | Action |
|---|---|---|---|---|---|
| Asymptomatic | Normal | Normal | Normal | True remission | Continue maintenance |
| Asymptomatic | Normal | Elevated | Normal | False positive FC | Reassure; no escalation |
| Asymptomatic | Normal | Elevated | Active (BWT >3 mm) | Subclinical inflammation | Consider escalation |
| Symptomatic | Normal | Normal | Normal | Functional symptoms | Treat functional symptoms |
| Symptomatic | Elevated | Elevated | Active | True inflammatory flare | Escalate anti-inflammatory therapy |
| Symptomatic (obstructive) | Normal | Normal | Stricture with prestenotic dilatation | Fibrostenotic disease | Consider dilation or surgery |
Note: IUS and biomarkers are complementary, not competitive. IUS provides anatomical localization, transmural assessment, and complication detection that biomarkers cannot offer. Combining both improves diagnostic accuracy and guides therapy more precisely than either alone.
References:
1. Maaser C, et al. Intestinal ultrasound for monitoring therapeutic response in patients with ulcerative colitis: results from the TRUST&UC study. Gut. 2020;69(9):1629-1636.
2. Dillman JR, et al. Defining the ultrasound longitudinal natural history of newly diagnosed pediatric small bowel Crohn disease treated with infliximab and infliximab-azathioprine combination therapy. Pediatr Radiol. 2017;47(8):924-934.
3. Furfaro F, et al. Noninvasive assessment of postoperative disease recurrence in Crohn’s disease: a multicenter, prospective cohort study. Clin Gastroenterol Hepatol. 2023;21(12):3143-3151.
4. Novak KL, et al. A simple ultrasound score for the accurate detection of inflammatory activity in Crohn’s disease. Inflamm Bowel Dis. 2017;23(11):2001-2010.
Treatment Escalation and De-escalation Based on IUS
- Therapy Escalation and De-escalation Based on IUS
- Clinical symptoms alone are unreliable for guiding therapy (up to 25% discordance with inflammation)
- Biomarkers (CRP, FC) cannot localize disease or detect complications
- Endoscopy is invasive and cannot be repeated frequently
- IUS provides real-time, non-invasive, transmural assessment that enables timely treatment adjustments
⎮”Symptoms of CD do not correlate well with the presence of active inflammation and therefore should not be the sole guide for therapy.”
📖ACG Clinical Guideline: Management of Crohn’s Disease in Adults (2025), Key Concept #9
When to Escalate Therapy Based on IUS
Click to expand/collapse table
| IUS Finding | Interpretation | Action |
|---|---|---|
| No response at 12–14 weeks (BWT reduction <25% or <2.0 mm) | Inadequate response to current therapy | Optimize dosing interval or dose; consider therapeutic drug monitoring |
| Worsening BWT or increased Limberg score | Disease progression despite treatment | Switch to alternative mechanism of action |
| New or worsening stricture with prestenotic dilatation (>3 cm) | Progressive fibrostenosis | Consider endoscopic balloon dilation or surgical referral |
| New abscess or fistula | Complicated penetrating disease | Antibiotics, percutaneous drainage, hold immunosuppression |
| Persistent active disease despite optimized therapy | Treatment failure | Change therapeutic class |
References:
1. Ilvemark JFKF, et al. Defining transabdominal intestinal ultrasound treatment response and remission in IBD: systematic review and expert consensus statement. J Crohns Colitis. 2022;16(4):554-580.
2. Ripollés T, et al. Ultrasonographic changes at 12 weeks of anti-TNF drugs predict 1-year sonographic response and clinical outcome in Crohn’s disease: a multicenter study. Inflamm Bowel Dis. 2016;22(10):2465-2473.
3. de Voogd F, et al. Intestinal ultrasound early on in treatment follow-up predicts endoscopic response to anti-TNFα treatment in Crohn’s disease. J Crohns Colitis. 2022;16(10):1598-1608.
4. Kucharzik T, et al. Use of intestinal ultrasound to monitor Crohn’s disease activity. Clin Gastroenterol Hepatol. 2017;15(4):535-542.e2.
When to De-escalate Therapy Based on IUS
De-escalation decisions should be individualized based on: disease history, prior complications (strictures, fistulas, surgery), patient preference, and risk of relapse.
Click to expand/collapse table
| IUS Finding | Interpretation | Action |
|---|---|---|
| Transmural remission (BWT ≤3 mm + absent Doppler signal) at 26–52 weeks | Deep healing achieved | Consider extending dosing interval or reducing dose |
| Sustained transmural remission for ≥6–12 months | Durable deep remission | Discuss de-escalation or drug holiday with shared decision-making |
| Normal IUS in asymptomatic patient on stable maintenance therapy | True remission | Continue current maintenance; monitor every 6–12 months |
References:
1. Ilvemark JFKF, et al. Defining transabdominal intestinal ultrasound treatment response and remission in IBD: systematic review and expert consensus statement. J Crohns Colitis. 2022;16(4):554-580.
2. Castiglione F, et al. One-year clinical outcomes with biologics in Crohn’s disease: transmural healing compared with mucosal or no healing. Aliment Pharmacol Ther. 2019;49(8):1026-1039.
3. Zorzi F, et al. Response assessed by ultrasonography as target of biological treatment for Crohn’s disease. Clin Gastroenterol Hepatol. 2020;18(9):2030-2037.
4. Calabrese E, et al. Ultrasonography tight control and monitoring in Crohn’s disease during different biological therapies: a multicenter study. Clin Gastroenterol Hepatol. 2022;20(3):e711-e722.
IUS-Guided Tight Control Algorithm
Click to expand/collapse table
| Timing | IUS Finding | Action |
|---|---|---|
| Baseline (pre-treatment) | Document BWT, Limberg score, complications | Benchmark for follow-up; select therapy based on severity and complications |
| Week 8–14 (post-induction) | Response: BWT reduction ≥25% or ≥2.0 mm | Continue therapy → reassess at week 26–52 |
| Week 8–14 (post-induction) | No response: minimal or no change | Optimize (dose/interval) or switch therapy |
| Week 26–52 (maintenance) | Transmural remission: BWT ≤3 mm + absent Doppler | Consider de-escalation (extend interval / reduce dose) |
| Week 26–52 (maintenance) | Persistent activity: BWT >3 mm or positive Doppler | Escalate or switch therapy |
| Every 6–12 months (surveillance) | Sustained transmural remission | Continue monitoring; consider further de-escalation |
| Every 6–12 months (surveillance) | New or worsening findings | Re-evaluate and adjust therapy |
References:
1. Ilvemark JFKF, et al. Defining transabdominal intestinal ultrasound treatment response and remission in IBD: systematic review and expert consensus statement. J Crohns Colitis. 2022;16(4):554-580.
2. Ripollés T, et al. Ultrasonographic changes at 12 weeks of anti-TNF drugs predict 1-year sonographic response and clinical outcome in Crohn’s disease: a multicenter study. Inflamm Bowel Dis. 2016;22(10):2465-2473.
3. Kucharzik T, et al. Use of intestinal ultrasound to monitor Crohn’s disease activity. Clin Gastroenterol Hepatol. 2017;15(4):535-542.e2.
4. Maaser C, et al. Intestinal ultrasound for monitoring therapeutic response in patients with ulcerative colitis: results from the TRUST&UC study. Gut. 2020;69(9):1629-1636.
5. de Voogd F, et al. Intestinal ultrasound early on in treatment follow-up predicts endoscopic response to anti-TNFα treatment in Crohn’s disease. J Crohns Colitis. 2022;16(10):1598-1608.
◾️Summary: IUS in Therapeutic Decision-Making
- IUS enables real-time, non-invasive, transmural assessment that:
- Guides escalation when the response is inadequate
- Guides de-escalation when deep remission is achieved
- Detects complications (strictures, fistulas, abscesses) early
- Reduces unnecessary endoscopy and radiation exposure
- Improves patient compliance and shared decision-making.
Clinical Case Example
Click to expand/collapse case example
Symptoms: Avoiding fibrous foods due to abdominal pain; 2–3 bowel movements daily; no blood, no urgency, no tenesmus
Last colonoscopy (2 years prior): Ulceration at ileocecal valve; terminal ileum not visualized due to stenosis
Current medications: Adalimumab + 6-mercaptopurine
| Without IUS | Timeline | With IUS (Point-of-Care) |
|---|---|---|
| Labs (CRP, CBC, drug level) ordered | 1 month later | IUS performed same day Findings: terminal ileum stricture with pre-stenotic dilation; colonic inflammation; increased BWT and hyperemia |
| Colonoscopy scheduled | ~2 months later | |
| MR enterography scheduled | 3 months later |
• Symptoms alone are unreliable – Patient had only mild symptoms but severe stricture and active inflammation on IUS
• IUS accelerates care – Decision to change therapy was made same day, not 1–3 months later
• IUS complements endoscopy – Colonoscopy failed to visualize the terminal ileum due to stenosis; IUS provided the missing information
• Patient-centered – No preparation, no sedation, no radiation, immediate results
References:
1. Friedman AB, et al. Effect of point-of-care gastrointestinal ultrasound on decision-making and management in inflammatory bowel disease. Aliment Pharmacol Ther. 2021;54(5):652-666.
2. Novak KL, et al. Clinic-based point of care transabdominal ultrasound for monitoring Crohn’s disease: impact on clinical decision making. J Crohns Colitis. 2015;9(9):795-801.
3. Dolinger MT, Kayal M. Intestinal ultrasound as a non-invasive tool to monitor inflammatory bowel disease activity and guide clinical decision making. World J Gastroenterol. 2023;29(15):2272-2282.
RECAP
- IUS is a non-invasive, radiation-free, real-time imaging tool that provides transmural assessment of IBD activity *.
- IUS is comparable to MRE and CTE for detecting disease activity and complications (strictures, fistulas, abscesses) *.
- IUS correlates well with endoscopy (r = 0.70–0.85) and is patient-preferred over repeated colonoscopies *,*.
- IUS adds value beyond clinical symptoms (which are unreliable in up to 25% of patients) and biomarkers (which cannot localize disease or detect complications) *, *.
- Transmural healing (BWT ≤3 mm + absent Doppler) is associated with lower rates of surgery, hospitalization, and corticosteroid use *.
- IUS enables early assessment of treatment response (as early as week 4–8) and guides therapy escalation or de-escalation in a tight control strategy *.
- IUS is particularly valuable in special populations: pregnancy (safe), pediatrics (no sedation), and postoperative CD (early recurrence detection) *.
- Limitations include operator dependency, limited visualization of rectum/proximal jejunum, and inability to screen for dysplasia *.
- IUS is not a replacement for endoscopy but a complementary tool that, when combined with symptoms and biomarkers, optimizes IBD management *.
- Intestinal ultrasound is a transformative, non-invasive tool that provides real-time, transmural assessment of IBD activity. When integrated into a tight-control monitoring strategy alongside clinical assessment and biomarkers, IUS enables earlier treatment optimization, reduces unnecessary endoscopy and radiation exposure, improves patient compliance, and is associated with better long-term outcomes, including lower rates of surgery and hospitalization.
Going Further
- US of the GI tract – Normal Anatomy (Radiology Assistant)
- Crohn’s disease – role of Ultrasound (Radiology assistant)
📚Guidelines
Appendix
📊Classification of available therapy for IBD
Click to expand/collapse table
| Drug Class / Mechanism | Agents | Approved Indications | Clinical Use / Severity |
|---|---|---|---|
| 5-Aminosalicylates (5-ASAs) (Topical anti-inflammatory) |
Mesalamine, Sulfasalazine, Olsalazine, Balsalazide Oral and rectal formulations |
UC (mild-to-moderate) CD (limited efficacy; not recommended per ACG 2025) |
First-line for mild-to-moderate UC (proctitis, left-sided, extensive) Rectal 5-ASA preferred for proctitis Not recommended for CD (ACG 2025 strong recommendation) |
| Corticosteroids (Systemic and topical) |
Prednisone, Methylprednisolone, Budesonide (CIR, MMX), Hydrocortisone | UC (mild-to-severe) CD (mild-to-severe) |
Short-term induction only (2–3 months) Budesonide for mild-to-moderate ileocecal CD or left-sided UC Not for maintenance (strong recommendation) Avoid in abscess/fistula |
| Immunomodulators – Thiopurines | Azathioprine (AZA), 6-Mercaptopurine (6-MP) | UC (maintenance) CD (maintenance, combination therapy) |
Not for induction (slow onset 8–12 weeks) Maintenance after steroid induction Combination with anti-TNF (reduces immunogenicity) TPMT/NUDT15 testing required |
| Immunomodulators – Methotrexate | Methotrexate (MTX) – IM/SC weekly | CD (maintenance) UC (limited efficacy – not recommended per ACG 2025) |
Maintenance in CD after steroid induction Not effective for induction in UC Combination with anti-TNF (alternative to thiopurines) |
| Anti-TNF Agents | Infliximab (IV/SC), Adalimumab (SC), Certolizumab pegol (SC), Golimumab (SC – UC only) | UC (moderate-to-severe) CD (moderate-to-severe) Perianal fistulizing CD |
First-line advanced therapy for moderate-to-severe IBD Infliximab preferred for UC and fistulizing CD Combination with immunomodulator recommended (infliximab) Monitor drug levels and antibodies |
| Anti-Integrins (Gut-selective) |
Vedolizumab (IV/SC) | UC (moderate-to-severe) CD (moderate-to-severe) |
Gut-selective, favorable safety profile Effective in anti-TNF exposed and naive patients Slower onset than anti-TNF SC formulation available for maintenance |
| Anti-IL12/23 (p40) | Ustekinumab (IV induction, SC maintenance) | CD (moderate-to-severe) UC (moderate-to-severe) |
Effective in anti-TNF refractory patients Favorable safety profile Dose optimization available for loss of response |
| Anti-IL23 (p19) | Risankizumab, Guselkumab, Mirikizumab | CD (moderate-to-severe) UC (moderate-to-severe) |
Newer class with rapid onset Risankizumab superior to ustekinumab in anti-TNF exposed CD (SEQUENCE trial) Guselkumab and mirikizumab approved for UC |
| JAK Inhibitors (Oral small molecules) |
Tofacitinib (non-selective), Upadacitinib (JAK1-selective) | UC (moderate-to-severe) Upadacitinib also for CD (after anti-TNF failure) |
Rapid onset (days to weeks) Oral administration Requires anti-TNF failure for UC (US label) Monitor for VTE, MACE, herpes zoster |
| S1P Receptor Modulators (Oral small molecules) |
Ozanimod (S1P1/5), Etrasimod (S1P1/4/5) | UC (moderate-to-severe) | Oral, gut-selective lymphocyte trapping Effective in anti-TNF experienced patients Etrasimod effective in isolated proctitis Monitor bradycardia, liver enzymes |
| Antibiotics (Limited role) |
Metronidazole, Ciprofloxacin | Perianal CD (adjunctive) Postoperative CD prophylaxis (low risk) |
Not effective for luminal CD (ACG 2025) Adjunctive for perianal fistulas with anti-TNF Postoperative prophylaxis (low risk, short-term) |
Notes:
• Mild-to-moderate UC: 5-ASA first-line (oral + rectal). Budesonide MMX for left-sided or extensive if 5-ASA fails.
• Moderate-to-severe UC: Anti-TNF, vedolizumab, ustekinumab, anti-IL23 (guselkumab, mirikizumab, risankizumab), JAK inhibitors (tofacitinib, upadacitinib), S1P modulators (ozanimod, etrasimod).
• Mild-to-moderate CD (ileocecal): Budesonide CIR 9 mg daily.
• Moderate-to-severe CD: Anti-TNF, vedolizumab, ustekinumab, anti-IL23 (risankizumab preferred after anti-TNF failure), upadacitinib (after anti-TNF failure).
• Perianal fistulizing CD: Anti-TNF (infliximab preferred), antibiotics as adjunct, surgical evaluation with seton placement.
• Postoperative CD: Anti-TNF for high-risk patients; metronidazole for low-risk (short-term).
References:
1. Lichtenstein GR, et al. ACG clinical guideline: management of Crohn’s disease in adults. Am J Gastroenterol. 2025;120(6):1225-1264.
2. Rubin DT, et al. ACG clinical guideline: ulcerative colitis in adults. Am J Gastroenterol. 2025;120(6):1187-1224.
3. Turner D, et al. STRIDE-II: an update on the selecting therapeutic targets in IBD. Gastroenterology. 2021;160(5):1570-1583.
📊Ileal Crohn’s vs. sigmoid/colon Crohn’s disease
Click to expand/collapse table
| Drug Class / Mechanism | Agents | Approved Indications | Clinical Use / Severity |
|---|---|---|---|
| 5-Aminosalicylates (5-ASAs) (Topical anti-inflammatory) |
Mesalamine, Sulfasalazine, Olsalazine, Balsalazide Oral and rectal formulations |
UC (mild-to-moderate) CD (limited efficacy; not recommended per ACG 2025) |
First-line for mild-to-moderate UC (proctitis, left-sided, extensive) Rectal 5-ASA preferred for proctitis Not recommended for CD (ACG 2025 strong recommendation) |
| Corticosteroids (Systemic and topical) |
Prednisone, Methylprednisolone, Budesonide (CIR, MMX), Hydrocortisone | UC (mild-to-severe) CD (mild-to-severe) |
Short-term induction only (2–3 months) Budesonide for mild-to-moderate ileocecal CD or left-sided UC Not for maintenance (strong recommendation) Avoid in abscess/fistula |
| Immunomodulators – Thiopurines | Azathioprine (AZA), 6-Mercaptopurine (6-MP) | UC (maintenance) CD (maintenance, combination therapy) |
Not for induction (slow onset 8–12 weeks) Maintenance after steroid induction Combination with anti-TNF (reduces immunogenicity) TPMT/NUDT15 testing required |
| Immunomodulators – Methotrexate | Methotrexate (MTX) – IM/SC weekly | CD (maintenance) UC (limited efficacy – not recommended per ACG 2025) |
Maintenance in CD after steroid induction Not effective for induction in UC Combination with anti-TNF (alternative to thiopurines) |
| Anti-TNF Agents | Infliximab (IV/SC), Adalimumab (SC), Certolizumab pegol (SC), Golimumab (SC – UC only) | UC (moderate-to-severe) CD (moderate-to-severe) Perianal fistulizing CD |
First-line advanced therapy for moderate-to-severe IBD Infliximab preferred for UC and fistulizing CD Combination with immunomodulator recommended (infliximab) Monitor drug levels and antibodies |
| Anti-Integrins (Gut-selective) |
Vedolizumab (IV/SC) | UC (moderate-to-severe) CD (moderate-to-severe) |
Gut-selective, favorable safety profile Effective in anti-TNF exposed and naive patients Slower onset than anti-TNF SC formulation available for maintenance |
| Anti-IL12/23 (p40) | Ustekinumab (IV induction, SC maintenance) | CD (moderate-to-severe) UC (moderate-to-severe) |
Effective in anti-TNF refractory patients Favorable safety profile Dose optimization available for loss of response |
| Anti-IL23 (p19) | Risankizumab, Guselkumab, Mirikizumab | CD (moderate-to-severe) UC (moderate-to-severe) |
Newer class with rapid onset Risankizumab superior to ustekinumab in anti-TNF exposed CD (SEQUENCE trial) Guselkumab and mirikizumab approved for UC |
| JAK Inhibitors (Oral small molecules) |
Tofacitinib (non-selective), Upadacitinib (JAK1-selective) | UC (moderate-to-severe) Upadacitinib also for CD (after anti-TNF failure) |
Rapid onset (days to weeks) Oral administration Requires anti-TNF failure for UC (US label) Monitor for VTE, MACE, herpes zoster |
| S1P Receptor Modulators (Oral small molecules) |
Ozanimod (S1P1/5), Etrasimod (S1P1/4/5) | UC (moderate-to-severe) | Oral, gut-selective lymphocyte trapping Effective in anti-TNF experienced patients Etrasimod effective in isolated proctitis Monitor bradycardia, liver enzymes |
| Antibiotics (Limited role) |
Metronidazole, Ciprofloxacin | Perianal CD (adjunctive) Postoperative CD prophylaxis (low risk) |
Not effective for luminal CD (ACG 2025) Adjunctive for perianal fistulas with anti-TNF Postoperative prophylaxis (low risk, short-term) |
Notes:
• Mild-to-moderate UC: 5-ASA first-line (oral + rectal). Budesonide MMX for left-sided or extensive if 5-ASA fails.
• Moderate-to-severe UC: Anti-TNF, vedolizumab, ustekinumab, anti-IL23 (guselkumab, mirikizumab, risankizumab), JAK inhibitors (tofacitinib, upadacitinib), S1P modulators (ozanimod, etrasimod).
• Mild-to-moderate CD (ileocecal): Budesonide CIR 9 mg daily.
• Moderate-to-severe CD: Anti-TNF, vedolizumab, ustekinumab, anti-IL23 (risankizumab preferred after anti-TNF failure), upadacitinib (after anti-TNF failure).
• Perianal fistulizing CD: Anti-TNF (infliximab preferred), antibiotics as adjunct, surgical evaluation with seton placement.
• Postoperative CD: Anti-TNF for high-risk patients; metronidazole for low-risk (short-term).
References:
1. Lichtenstein GR, et al. ACG clinical guideline: management of Crohn’s disease in adults. Am J Gastroenterol. 2025;120(6):1225-1264.
2. Rubin DT, et al. ACG clinical guideline: ulcerative colitis in adults. Am J Gastroenterol. 2025;120(6):1187-1224.
3. Turner D, et al. STRIDE-II: an update on the selecting therapeutic targets in IBD. Gastroenterology. 2021;160(5):1570-1583.
📽️Media
- Paralytic ileus
- Patient with acute appendicitis and peritonitis, showing a dilated jejunum (> 3 cm) with clear fluid content and without peristaltic activity of contractions over a length of> 10 cm
- Intestinal Ultrasound for IBD Monitoring
References
1. PMID: 40701562. Lichtenstein GR, Loftus EV, Afzali A, Long MD, Barnes EL, Isaacs KL, Ha CY. ACG Clinical Guideline: Management of Crohn’s Disease in Adults. Am J Gastroenterol. 2025 Jun 3;120(6):1225-1264. doi: 10.14309/ajg.0000000000003465.
2. PMID: 40701556. Rubin DT, Ananthakrishnan AN, Siegel CA, Barnes EL, Long MD. ACG Clinical Guideline Update: Ulcerative Colitis in Adults. Am J Gastroenterol. 2025 Jun 3;120(6):1187-1224. doi: 10.14309/ajg.0000000000003463.
3. PMID: 25590387. Muradali D, Goldberg DR. US of gastrointestinal tract disease. Radiographics. 2015 Jan-Feb;35(1):50-68. doi: 10.1148/rg.351140003.
4. Felicani C, Trovati A, Franchi E, Zanni F, Verzelloni F, Bianchini A, et al. Transabdominal Gastro-Intestinal UltraSound (GIUS): a visual approach to intestinal pathology. Explor Dig Dis. 2024;3:241–61. https://doi.org/10.37349/edd.2024.00050
5. PMID: 29097866. Atkinson NSS, et al. . How to perform gastrointestinal ultrasound: Anatomy and normal findings. World J Gastroenterol. 2017 Oct 14;23(38):6931-6941. doi: 10.3748/wjg.v23.i38.6931.
6. PMID: 36087155. Nishida M, Hasegawa Y, Hata J. Basic practices for gastrointestinal ultrasound. J Med Ultrason (2001). 2023 Jul;50(3):285-310. doi: 10.1007/s10396-022-01236-0. Epub 2022 Sep 10. Erratum in: J Med Ultrason (2001). 2023 Jul;50(3):311. doi: 10.1007/s10396-023-01339-2
7. PMID: 27604052. Nylund K, et al. EFSUMB Recommendations and Guidelines for Gastrointestinal Ultrasound. Ultraschall Med. 2017 Jun;38(3):e1-e15. English. doi: 10.1055/s-0042-115853. Epub 2016 Sep 7.
8. PMID: 33808245. Rosano N, et al. Ultrasound of Small Bowel Obstruction: A Pictorial Review. Diagnostics (Basel). 2021 Mar 30;11(4):617. doi: 10.3390/diagnostics11040617.
9. PMID: 35213095. Hata J, Imamura H. The Use of Transabdominal Ultrasound in Inflammatory Bowel Disease. Korean J Radiol. 2022 Mar;23(3):308-321. doi: 10.3348/kjr.2021.0692.
10. PMID: 40030691. Petersen F, Höpfner MH, Jenssen C, Nürnberg D, Strobel D, Vogelpohl J, Dietrich CF. Why is ultrasound needed in inflammatory bowel disease? Med Ultrason. 2025 Dec 12;27(4):440-449. doi: 10.11152/mu-4492. Epub 2025 Feb 26.
11. PMID: 34357022. Furfaro F, et al. Bowel Ultrasound in Inflammatory Bowel Disease: How Far in the Grayscale? Life (Basel). 2021 Jul 4;11(7):649. doi: 10.3390/life11070649.
12. PMID: 39510664. Medellin A, Wilson SR. Bowel Ultrasound. Radiol Clin North Am. 2025 Jan;63(1):83-96. doi: 10.1016/j.rcl.2024.08.002. Epub 2024 Oct 2.
13. PMID: 35677820. Nardone OM, et al. The Impact of Intestinal Ultrasound on the Management of Inflammatory Bowel Disease: From Established Facts Toward New Horizons. Front Med (Lausanne). 2022 May 23;9:898092. doi: 10.3389/fmed.2022.898092.
14. PMID: 29437914. Bryant RV, et al. Gastrointestinal ultrasound in inflammatory bowel disease: an underused resource with potential paradigm-changing application. Gut. 2018 May;67(5):973-985. doi: 10.1136/gutjnl-2017-315655.
15. PMID: 39415376. Kumar R, Melmed GY, Gu P. Imaging in Inflammatory Bowel Disease. Rheum Dis Clin North Am. 2024 Nov;50(4):721-733. doi: 10.1016/j.rdc.2024.07.009. Epub 2024 Aug 26.
16. PMID: 30991429. Kunze G, Seitz K, Mauch M, Petersen F. Clinical Ultrasound in Inflammatory Bowel Disease. Ultraschall Med. 2019 Apr;40(2):132-162. English. doi: 10.1055/a-0869-8799. Epub 2019 Apr 16.
17. PMID: 33367962. Goertz RS, Hensel S, Wildner D, Neurath MF, Strobel D. Bowel wall thickening and hyperemia assessed by high-frequency ultrasound indicate histological inflammation in Crohn’s ileitis. Abdom Radiol (NY). 2021 May;46(5):1855-1863. doi: 10.1007/s00261-020-02895-8. Epub 2020 Dec 24.
18. PMID: 40488637. Gaidos JKJ, Hashash JG. Monitoring Inflammatory Bowel Disease Activity: When, How, and Why. Am J Gastroenterol. 2025 Jun 9;120(8):1732-1741. doi: 10.14309/ajg.0000000000003582.
19. PMID: 39001773. Chavannes M, Dolinger MT, Cohen-Mekelburg S, Abraham B. AGA Clinical Practice Update on the Role of Intestinal Ultrasound in Inflammatory Bowel Disease: Commentary. Clin Gastroenterol Hepatol. 2024 Sep;22(9):1790-1795.e1. doi: 10.1016/j.cgh.2024.04.039. Epub 2024 Jul 10.
20. PMID: 35132795. Christian M, Giovanni M, Torsten K, Mariangela A. Ultrasonography in inflammatory bowel disease – So far we are? United European Gastroenterol J. 2022 Mar;10(2):225-232. doi: 10.1002/ueg2.12196. Epub 2022 Feb 8. Erratum in: United European Gastroenterol J. 2022 May;10(4):439. doi: 10.1002/ueg2.12225.
21. PMID: 37124889. Dolinger MT, Kayal M. Intestinal ultrasound as a non-invasive tool to monitor inflammatory bowel disease activity and guide clinical decision making. World J Gastroenterol. 2023 Apr 21;29(15):2272-2282. doi: 10.3748/wjg.v29.i15.2272.
22. PMID: 22109321. Maturen KE, Wasnik AP, Kamaya A, Dillman JR, Kaza RK, Pandya A, Maheshwary RK. Ultrasound imaging of bowel pathology: technique and keys to diagnosis in the acute abdomen. AJR Am J Roentgenol. 2011 Dec;197(6):W1067-75. doi: 10.2214/AJR.11.6594.
23. PMID: 40741688. Kucharzik T, et al. ECCO-ESGAR-ESP-IBUS Guideline on Diagnostics and Monitoring of Patients with Inflammatory Bowel Disease: Part 1. J Crohns Colitis. 2025 Jul 3;19(7):jjaf106. doi: 10.1093/ecco-jcc/jjaf106.
24. PMID: 41173014. Eggermont E, et al. Ulcerative colitis: moving beyond the mucosal dogma. Lancet Gastroenterol Hepatol. 2026 Feb;11(2):163-174. doi: 10.1016/S2468-1253(25)00263-8. Epub 2025 Oct 28. PMID: 41173014.
25. PMID: 36514508. Limbri LF, Wilson TG, Oliver MR. Prevalence of irritable bowel syndrome and functional abdominal pain disorders in children with inflammatory bowel disease in remission. JGH Open. 2022 Nov 3;6(12):818-823. doi: 10.1002/jgh3.12791.
26. PMID: 40488637. Gaidos JKJ, Hashash JG. Monitoring Inflammatory Bowel Disease Activity: When, How, and Why. Am J Gastroenterol. 2025 Jun 9;120(8):1732-1741. doi: 10.14309/ajg.0000000000003582.
Shahriar Lahouti
You may also like
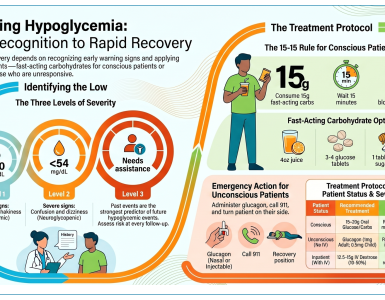
Hypoglycemia-Diagnosis and Treatment in Adult Patients
Dec 23, 2021 via Shahriar Lahouti. Updated 30 June 2026. CONTENTS Preface Etiology Background Cuases Risk factors Antidiabetic Medications Mechanism of action Non-insulin Anti-diabetic agents Insulin Insulin- Rapid...

Update on Management of Acute Ischemic Stroke in The Emergency Department
24 September 2021, via Shahriar Lahouti. Last Update 13 June 2026. CONTENTS Preface Pathophysiology of stroke Physiology: Core infarct vs. ischemic Penumbra Clinical presentation Anatomy of stroke Arterial territories...

A Practical Guide to Read Chest CT For Emergency and Critical Care Physicians
2 May 2026 by Shahriar Lahouti. CONTENTS Preface PART I: The foundation & systemic approach Technical Essentials Hounsfield Units Contrast Timing & Protocols Windows Cardiac anatomy The 60-Second Systematic...

RECAPEM stands For Rational Evidence, Changing Academic Practice in Emergency
Medicine. We cover plenty of challenging topics in the field of emergency medicine and
critical care.
Copyright © 2026 · powered by MedoLink.dev
Add comment