


Dec 20, 2021 via Shahriar Lahouti
Introduction
Dizziness is an imprecise term and a common symptom of many disease processes. The chief complaints of dizziness, imbalance, vertigo or lightheadedness account for roughly 4% of all United States ED visits. Sometimes it is challenging to differentiate the benign from dangerous causes of vertigo in ED.
In this post, a rapid guide on differentials and diagnostic approach to vertigo is outlined.
👉Distinguishing the “type” of dizziness by descriptive quality (i.e. vertigo, disequilibrium or presyncope) is inconsistent and a common source of diagnostic error.
👉Focus on the Timing, Triggers and Associated Symptoms during the patient interview in an effort to improve diagnostic accuracy and reduce diagnostic error.
- The ATTEST mnemonic was created to help remind providers to think broadly and systematically with undifferentiated dizzy patients:
-
-
A (associated symptoms)
-
T (timing)
-
T (triggers)
-
ES (exam signs)
-
T (testing)
-
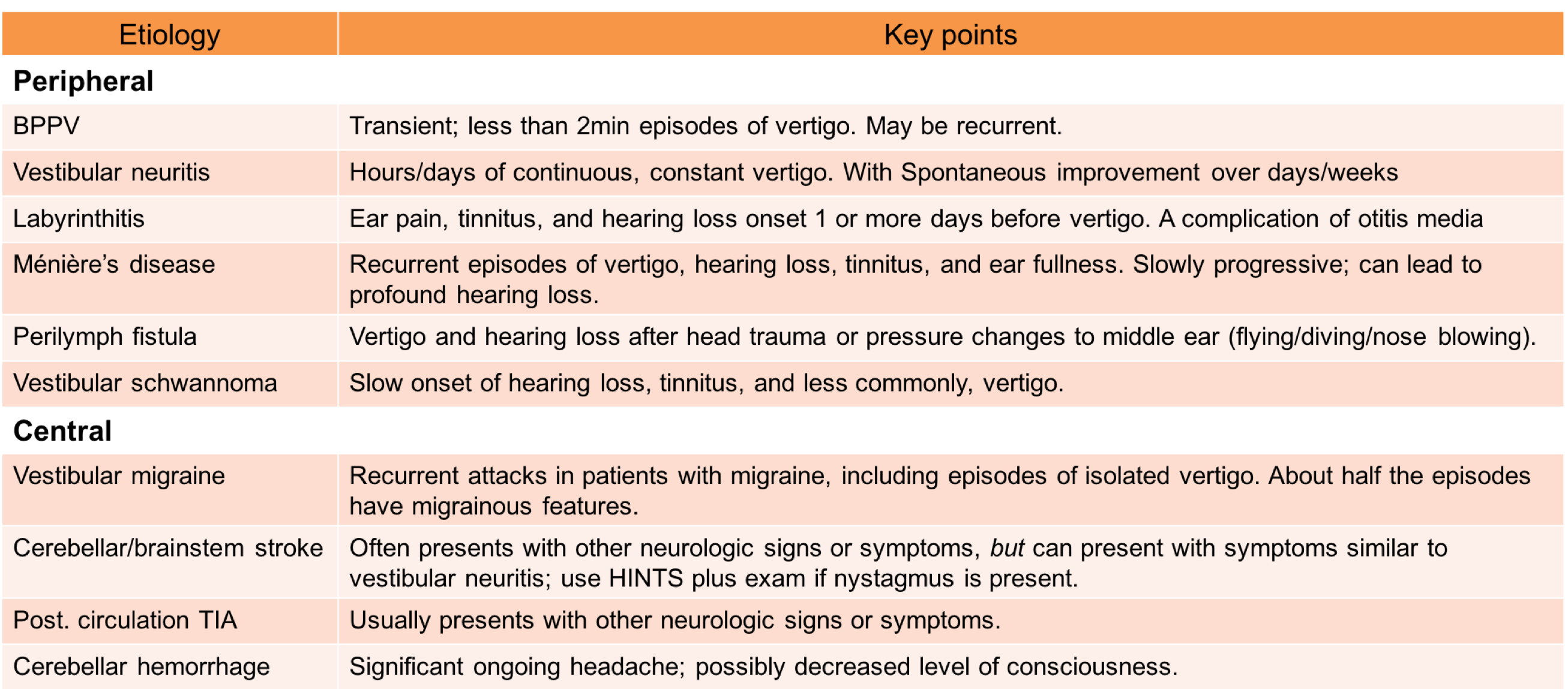
Keep in mind that brainstem and posterior fossa stroke can manifest as abrupt onset of vertigo.
- Patients with stroke commonly have additional symptoms, although isolated vertigo is shown to happen in 0.7% of patients with brainstem stroke.
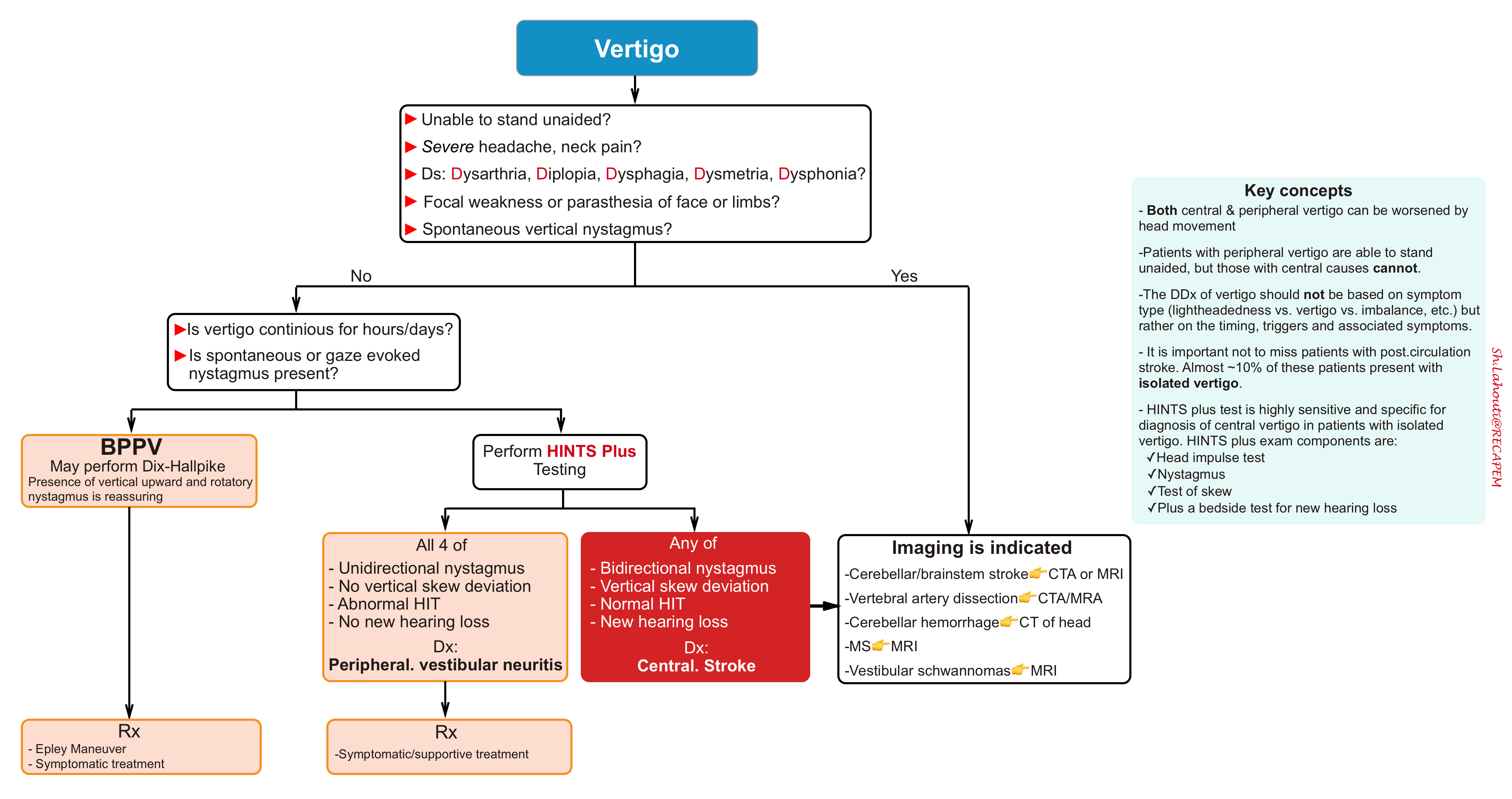
- The Head impulse, nystagmus, test of skew exam (HINTS) was developed and validated among neuro-otologists, where it was shown to outperform early MRI in the diagnosis of stroke among acutely dizzy patients.
- The Plus component of the HINTS plus exam (see the following algorithm) involves checking for acute hearing loss by rubbing thumb and index fingers together just lateral to the patient’s left and right ear and asking whether the patient can hear it. New hearing loss is suggestive for a central cause.
- A complete neurologic examination including assessment for posterior circulation is warranted. Check for
- Diplopia – any double vision on extraocular movement testing (CNs III, IV, VI)
- Dysarthria – any difficulty in speaking or facial asymmetry (CN VII)
- Dysphagia – any difficulty in swallowing (CNs IX and X)
- Dysmetria – (e.g. ataxia) any cerebellar findings (finger-to-nose, heel-to-shin, postural instability).
- Gait – A formal test of gait, both truncal (sitting up in the stretcher) and walking, should be performed.
- Patients with peripheral vertigo can present quite dramatically and they may appear hesitant or a little unsteady when walking, but they should be able to walk.
- Those who are unable to walk should be assumed to have a central process.
- Weakness/Sensory loss – any extremity findings from the descending tracts that pass through the brainstem en route to the body
Diagnostic approach to vertigo is shown in following algorithm.
HINTS exam
References
1. Edlow JA. A New Approach to the Diagnosis of Acute Dizziness in Adult Patients. Emerg Med Clin North Am. 2016 Nov;34(4):717-742. doi: 10.1016/j.emc.2016.06.004. Epub 2016 Sep 7. PMID: 27741985.
2. Kattah JC, Talkad AV, Wang DZ, Hsieh YH, Newman-Toker DE. HINTS to diagnose stroke in the acute vestibular syndrome: three-step bedside oculomotor examination more sensitive than early MRI diffusion-weighted imaging. Stroke. 2009 Nov;40(11):3504-10. doi: 10.1161/STROKEAHA.109.551234. Epub 2009 Sep 17. PMID: 19762709; PMCID: PMC4593511.
3. Newman-Toker DE, Edlow JA. TiTrATE: A Novel, Evidence-Based Approach to Diagnosing Acute Dizziness and Vertigo. Neurol Clin. 2015 Aug;33(3):577-99, viii. doi: 10.1016/j.ncl.2015.04.011. PMID: 26231273; PMCID: PMC4522574.

Add comment